Clear Sky Science · en
Machine-actionable criteria chart the symptom space of mental disorders
Why turning words into rules matters
Diagnosing mental health conditions relies on long, carefully negotiated manuals like the DSM-5. These books describe which symptom combinations count as disorders, but they do so in narrative prose, not in a form computers can directly use. This article shows how to translate those written rules into an exact, machine-readable map of all possible symptom patterns. That map reveals where diagnostic categories are cleanly separated, where they blur into each other, and how new proposals such as Long COVID fit—or fail to fit—within existing concepts.
From text on a page to a structured map
The authors start by treating diagnostic manuals as rule books that can, in principle, be written in a formal logical language. Each disorder is defined by criteria such as “at least five of nine symptoms, including either depressed mood or loss of interest.” From such sentences they extract the list of symptoms, the required numbers, and how those pieces are combined with “and/or” logic. They then encode every valid criteria-satisfying symptom combination—the full range of symptom profiles that would meet the written rules for a diagnosis. Each combination becomes a binary pattern indicating which symptoms are present, absent, or irrelevant for that disorder. Taken together, these patterns form a high‑dimensional “symptom space” that can be analyzed mathematically.
Testing whether diagnoses can be kept apart
With this map in hand, the authors ask a basic but rarely formalized question: can two disorders be distinguished purely on the basis of their official criteria? They introduce two tests. First, there should be no single symptom pattern that simultaneously fulfills both definitions; otherwise, the rules themselves would make the diagnoses indistinguishable. Second, no disorder’s minimal symptom pattern should be a strict subset of another’s, because that would mean one definition is simply a looser version of the other. Using toy examples, they show how these situations appear as overlapping or nested regions in symptom space, and they illustrate that some apparent overlaps in real patients reflect true co‑occurrence of different rule sets, not flaws in the definitions.
What the map reveals about known disorders
The framework is then applied to real DSM‑5 categories. For a group of schizophrenia‑spectrum disorders, the authors convert all narrative rules into formal combinations and compute a measure of similarity based on how close the allowed symptom patterns are. As expected, schizophrenia and schizophreniform disorder look very similar, because they share most core symptoms and mainly differ in how long those symptoms must last. Yet the formal tests show that their regions in symptom space do not share identical or nested minimal patterns. Visualizing these combinations in two dimensions confirms that, despite overlap in content, the criteria carve out distinct areas. This suggests that, at least for these examples, the current definitions are logically coherent and support meaningful differential diagnosis.
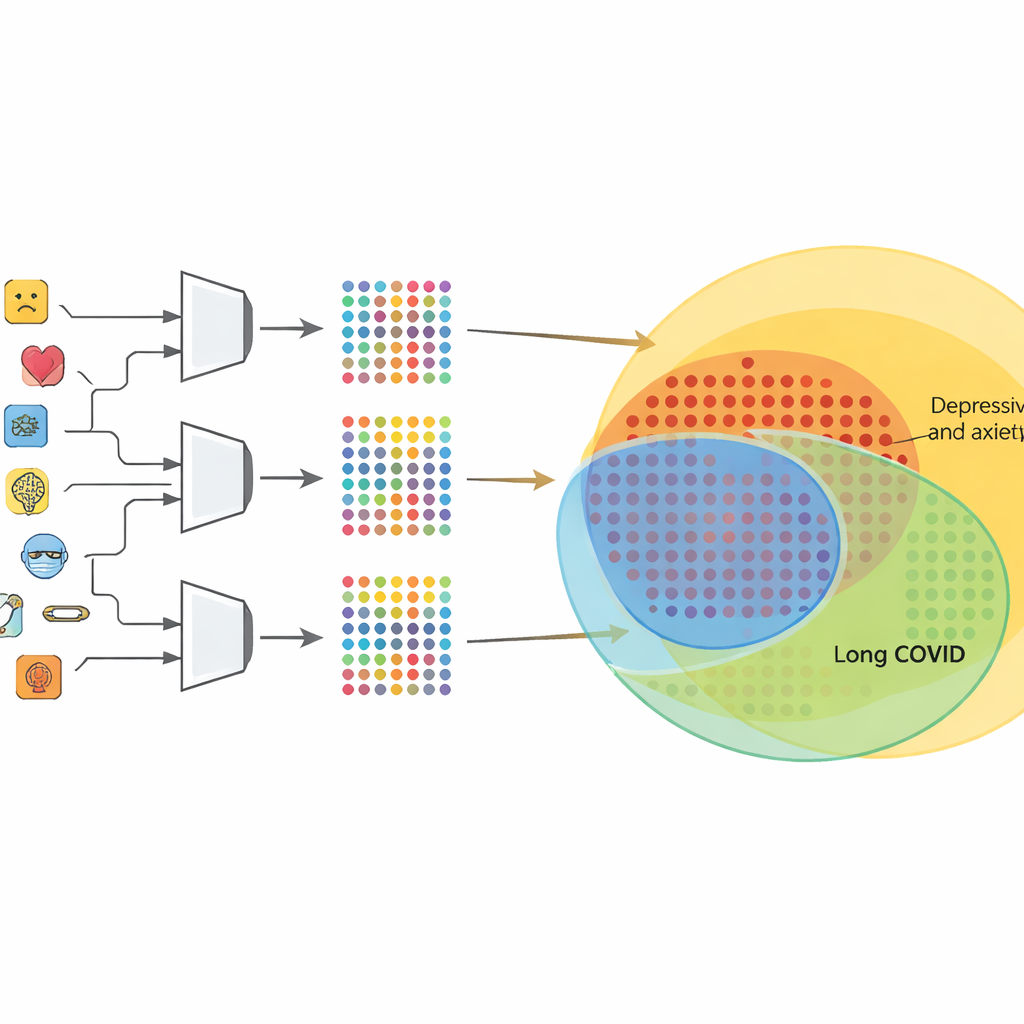
Where Long COVID blurs into mood and anxiety
The same method becomes more provocative when applied to Long COVID, using a recent consensus description that lists common ongoing symptoms such as fatigue, cognitive problems, sleep disturbance, and mood changes. After harmonizing the wording with DSM‑style symptom names, the authors generate all Long COVID–compatible patterns and compare them with those of several existing disorders. They find virtually no connection to psychotic conditions or speech disorders, but very strong structural similarity to major depression, persistent depression, panic disorder, and generalized anxiety. Crucially, an overwhelming majority of the valid patterns for these mood and anxiety disorders also satisfy the Long COVID symptom list. That means the proposed Long COVID definition is largely contained within already established categories, even if no single pattern is exactly identical.
How a computable consensus can guide future care
By turning narrative diagnostic rules into explicit, checkable structures, this work offers a transparent way to test whether new diagnoses truly add something conceptually distinct. For Long COVID, the analysis implies that symptom lists alone, without extra constraints such as timing, biological markers, or exclusion rules, are too broad to keep it separate from depression and anxiety. More generally, the method shows that as manuals accumulate more categories and criteria, unaided human reasoning cannot reliably track all the permitted combinations. A machine‑actionable, rule‑based map of the symptom space can help expert panels refine definitions, support clinicians with interpretable decision tools, and reduce the risk that diagnostic systems drift away from the very consensus they are meant to embody.
Citation: Strasser-Kirchweger, B., Kutil, R.H., Zimmermann, G. et al. Machine-actionable criteria chart the symptom space of mental disorders. npj Digit. Med. 9, 271 (2026). https://doi.org/10.1038/s41746-026-02451-6
Keywords: diagnostic criteria, mental health classification, computable medicine, Long COVID symptoms, clinical decision support