Clear Sky Science · en
Neuroimaging outcomes in suspected papilledema
Why eye swelling can signal hidden brain trouble
Papilledema, a type of swelling at the back of the eye, can be one of the body’s earliest warnings that pressure is building inside the skull. That pressure may come from treatable but sometimes life‑threatening problems like brain tumors, fluid buildup, or clots in the veins that drain the brain. This study asks a practical question that matters to anyone who might land in an emergency room with headache and eye changes: when doctors suspect papilledema, how often does brain imaging actually find something serious, and can symptoms alone tell who really needs a scan?
Who was studied in the emergency setting
Researchers in Berlin looked back at records from two large hospitals over 13 years, identifying 225 adults sent to the emergency department because eye doctors worried about papilledema. Everyone had a detailed eye exam and brain scans with CT or MRI, often along with a spinal tap to measure fluid pressure. The team then sorted patients into groups: those with true papilledema caused by high pressure in the skull, those whose optic nerve swelling came from other eye or nerve diseases, those with harmless look‑alike changes called pseudopapilledema, and a smaller group with incomplete testing.
What doctors actually found on brain scans
More than half of the patients did turn out to have papilledema. In most of these, the cause was idiopathic intracranial hypertension, a condition where pressure is high but no mass or blockage is seen. However, in about one in five of all patients, scans revealed more dangerous problems such as brain tumors, fluid buildup in the brain’s cavities, or clots in the draining veins. Both CT and MRI were quite effective at spotting these secondary causes, with MRI performing slightly better and requiring fewer scans to find one serious case. At the same time, about a third of patients had no raised pressure at all, even though their optic discs looked swollen at first glance.
Symptoms that mislead more than they guide
Headache, often thought of as a classic warning sign, was very common across nearly all groups and did not help doctors distinguish between dangerous and less dangerous causes. Blurred vision, vertigo, and how sharp the sight measured on eye charts were also surprisingly poor guides. Certain features did tilt the odds: people who had double vision, nausea and vomiting, or obvious new weaknesses in eye movements or other nerves were more likely to harbor tumors, fluid buildup, or vein clots. Still, many patients with serious brain disease had no clear focal neurological deficits, meaning that relying on symptoms alone would miss a substantial number of important findings.
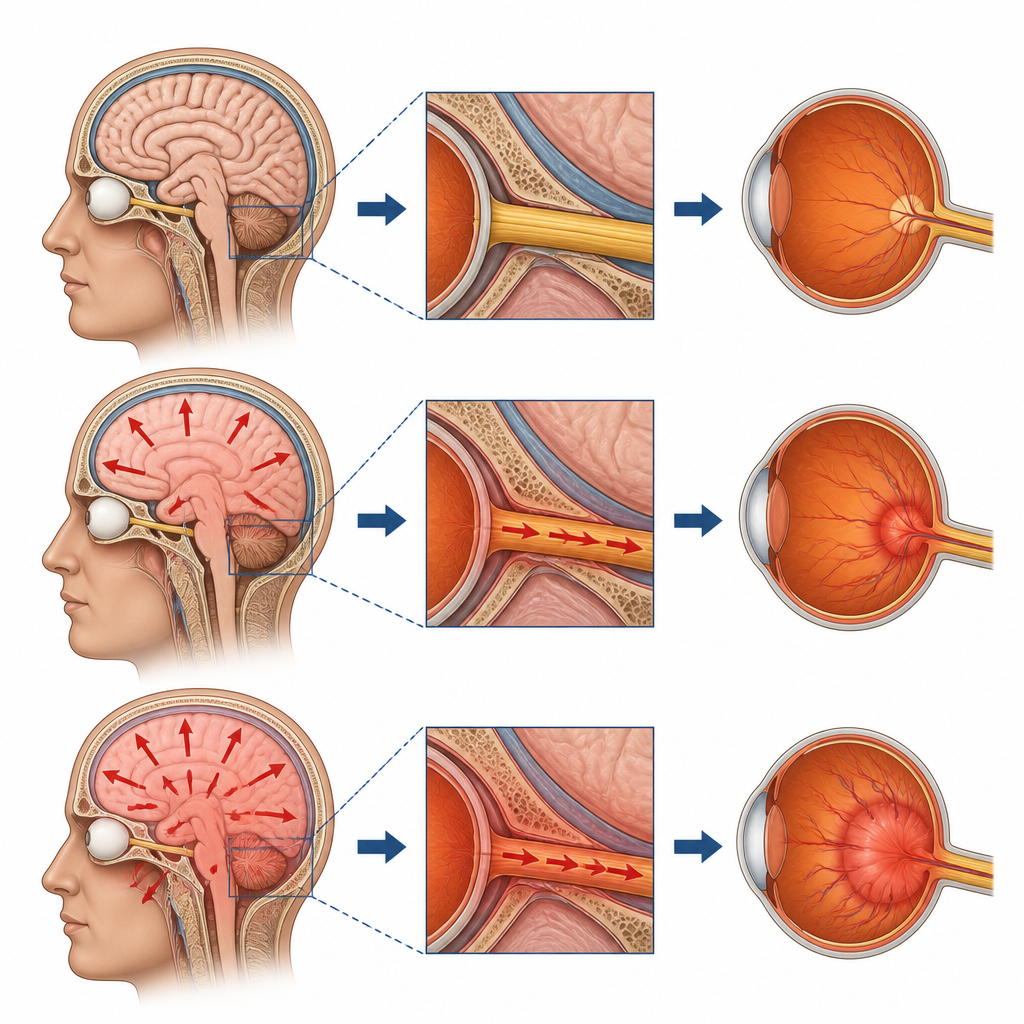
Clues from MRI and the limits of imaging signs
MRI sometimes showed patterns that fit with idiopathic intracranial hypertension, such as a slightly flattened back of the eye or widened fluid spaces around the optic nerves. These features strengthened the case for raised pressure when combined with a high spinal fluid reading and the right clinical picture. Yet they were far from perfect: some patients with this pressure disorder had no such signs, while similar patterns appeared in people with other illnesses or even as incidental findings. The study also found that a significant fraction of patients labeled with papilledema by referral actually had other optic nerve problems like inflammation, poor blood flow, or long‑standing structural quirks of the nerve.
What this means for patients with suspected eye swelling
For adults who arrive in the emergency department with suspected papilledema, this research shows that serious brain conditions are common enough, and symptoms are nonspecific enough, that routine brain imaging is warranted. Instead of trying to pick a “high‑risk” minority based only on complaints and the bedside exam, the authors argue that all such patients should receive timely scanning, ideally MRI including a focus on the brain’s veins, while minimizing unnecessary radiation from CT. In simple terms, when the back of the eye looks suspiciously swollen, a brain scan is usually the safest path to rule out hidden pressure problems and guide appropriate treatment.
Citation: Knoche, T., Guelsoy, N., Pietrock, C. et al. Neuroimaging outcomes in suspected papilledema. Sci Rep 16, 16372 (2026). https://doi.org/10.1038/s41598-026-55133-4
Keywords: papilledema, brain imaging, idiopathic intracranial hypertension, optic nerve swelling, emergency neurology