Clear Sky Science · en
Lateral reinforcement of anastomoses enhances mechanical strength in fragile neonatal oesophageal tissue
Stronger stitches for fragile newborn organs
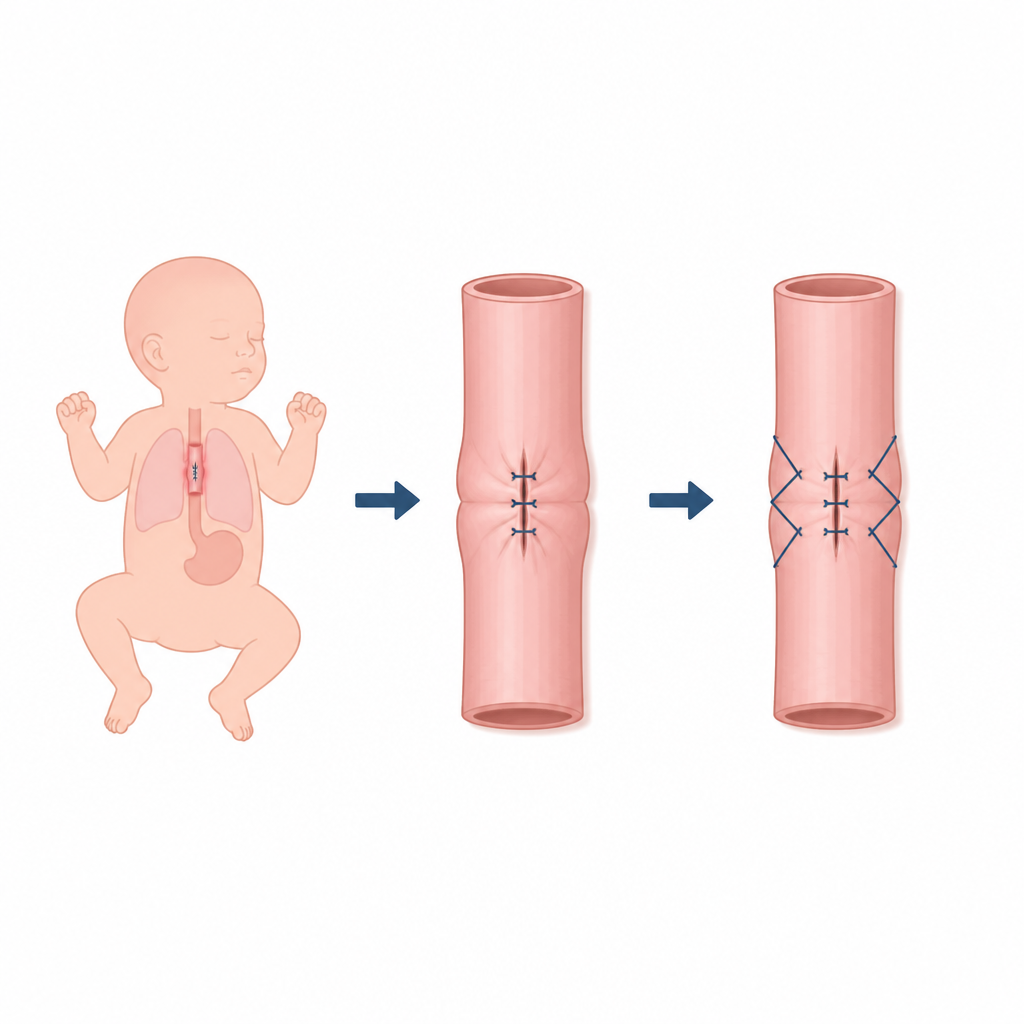
When babies are born with a broken food pipe their survival can depend on stitches just a few millimetres wide. In these tiny patients the tissue is soft and fragile and pulling the two ends together so they can swallow normally risks tearing the join and leaking stomach contents into the chest. This study asks a simple but vital question: can a small change in how surgeons place their stitches make that join safer without adding devices or complex materials?
Why joins in the food pipe can fail
Newborns with oesophageal atresia are born with a gap in the tube that carries food from the mouth to the stomach. Surgeons reconnect the ends, but the tissue is thin and under tension as the gap is closed. If the pull on a stitch is too strong or focused in one spot the wall can split lengthwise and allow fluid to leak out. Past research has shown that higher tension at the join sharply raises the risk of leaks, yet there has been little direct testing of how a single stitch starts a tear in such fragile tissue.
A simple extra stitch at the side
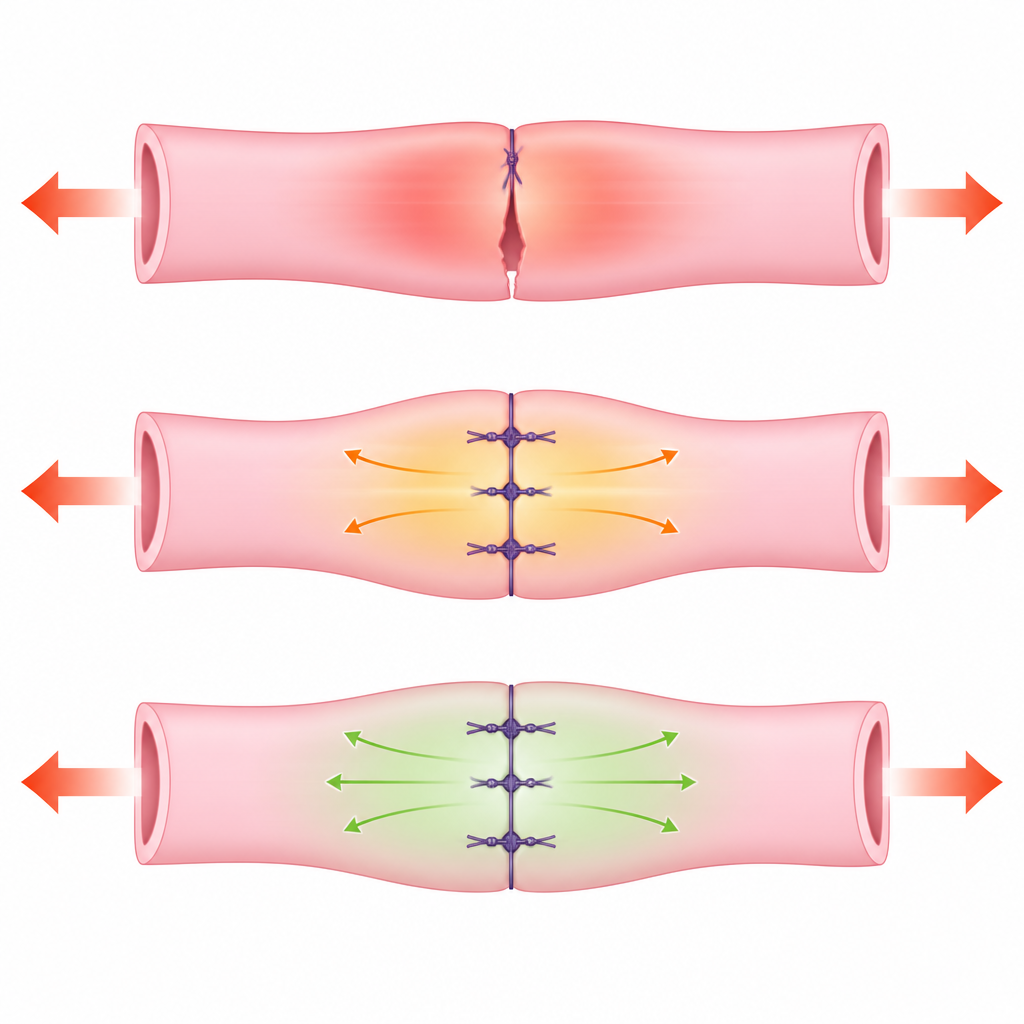
The team tested a small change called lateral reinforcement. Instead of relying on one main stitch to hold the edges, they added a short supporting stitch alongside it that spreads the load over a wider area of tissue. First they built an artificial model of the food pipe from a soft layered gel that stretches and tears like newborn tissue. Then they repeated the tests using rat intestine, which also behaves like a delicate tube. In both models they compared standard stitches with and without the side reinforcement and measured how much pulling force was needed before the tissue started to rip.
How much stronger the join became
In the gel model, the reinforced stitches needed about three and a half times more force to cause tearing than ordinary stitches. In the animal tissue they were more than twice as strong. The reinforced joins also tolerated a much larger stretch before failing, showing that the extra side stitch helped share the strain rather than letting it concentrate along a narrow line. Motion tracking of tiny marks on the model confirmed that the surrounding tissue moved more evenly when lateral reinforcement was used, which matches the idea that the load is spread out instead of focused on one weak point.
Putting the idea to work in real surgery
The authors then used the technique during keyhole operations in six newborns whose food pipe tore lengthwise while being stitched. In each case they first closed the tear and then added the deeper side reinforcement stitch to stop the rip from spreading. None of these babies developed a leak after surgery, even though the joins were under noticeable tension and the tissues were fragile. Several of the children later developed narrow spots at the join that needed stretching with a balloon, a known issue in this condition, but all eventually fed by mouth normally.
What this means for tiny patients
For parents and surgeons alike, the main message is that a modest change in sewing pattern can make a delicate join in a newborn’s food pipe much harder to tear. Lateral reinforcement does not remove the need for careful technique or further study, and larger groups of patients are needed to see how it affects long term narrowing of the tube. Still, the work shows in clear mechanical tests and early clinical use that adding a small side stitch can spread tension, strengthen the join, and may help reduce one of the most feared complications in this life saving surgery.
Citation: Guo, Y., Yasui, A., Takimoto, A. et al. Lateral reinforcement of anastomoses enhances mechanical strength in fragile neonatal oesophageal tissue. Sci Rep 16, 15820 (2026). https://doi.org/10.1038/s41598-026-47287-y
Keywords: esophageal atresia, neonatal surgery, suture technique, anastomotic leakage, tissue biomechanics