Clear Sky Science · en
Immunometabolic determinants of hepatitis B vaccine seroprotection among Ethiopian adults
Why this research matters
Many people assume that once they finish a vaccine series they are fully protected. This study of Ethiopian healthcare workers shows that the story is more complicated: the state of the body, especially blood fats and low-grade inflammation, can quietly weaken the shield that a hepatitis B vaccine is supposed to provide. Understanding these hidden influences can help keep frontline workers, and eventually the wider public, safer from a virus that still causes serious liver disease.
Lingering risk after vaccination
Hepatitis B virus is a major cause of cirrhosis and liver cancer around the world, and Ethiopia is among the countries where it remains common. Adults at high risk, such as healthcare providers, receive the full three-dose vaccine series. Yet when the researchers measured protective antibodies in 422 vaccinated healthcare workers from hospitals in northwestern Ethiopia, they found that about one in four did not have antibody levels considered protective. This shortfall raises concern that routine vaccination, while essential, may not be enough for everyone in settings where infection pressure is high.
The role of blood fats and quiet inflammation
The team focused on two sets of internal factors that might explain why some vaccinated adults remained vulnerable: blood lipids, which include “good” and “bad” cholesterol, and markers of ongoing inflammation. From small blood samples, they measured several types of cholesterol and fats, as well as C reactive protein, a common inflammation marker, and a newer combined index that reflects the balance between defensive and inflammatory blood cells. They also recorded body weight, diet and physical activity, along with age and other background information, to see how all these features lined up with the presence or absence of protective antibodies.
What the numbers revealed
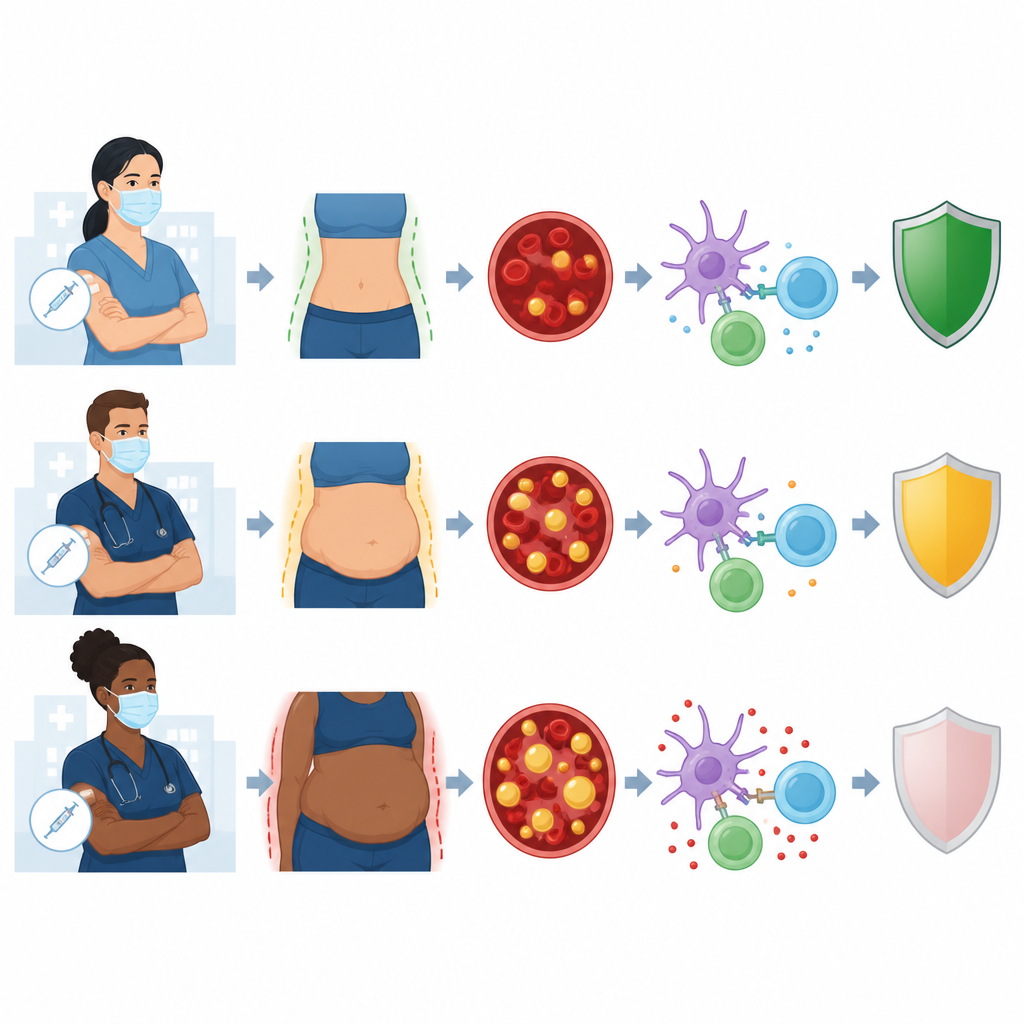
Overall, 73.7 percent of the participants had protective antibody levels, with middle aged adults making up the largest share of those protected. People with a normal body weight, a self reported healthy diet, and normal levels of the “good” cholesterol tended to be protected more often, although these trends were not strong enough to rule out chance when other factors were considered. In contrast, a high level of “bad” cholesterol stood out even after careful statistical adjustment: healthcare workers with raised low density lipoprotein were more likely to have weak protection. A composite inflammation score called the systemic immune inflammatory index showed an even clearer link, with high values tied to a markedly higher chance of lacking protective antibodies.
Beyond single risk factors
Some signals faded when the researchers adjusted for overlapping influences. For example, high triglycerides and an elevated C reactive protein level each seemed to predict poor protection at first glance, but their effects were no longer clear once age, weight and other lipids were taken into account. The stronger and more consistent patterns came from high “bad” cholesterol and the composite inflammation index, suggesting that it is the combined load of disrupted fat metabolism and smoldering immune activity that undermines how well the vaccine response is maintained, rather than any single marker alone.
What this means for everyday health
For a layperson, the key message is that vaccination is vital but not the whole story. In this group of Ethiopian healthcare workers, most were protected, yet those with high “bad” cholesterol and signs of chronic inflammation were more likely to have a weaker shield against hepatitis B despite being fully vaccinated. The findings hint that checking and improving blood fat levels and quiet inflammation could help vaccines do their job better, especially for adults living and working where hepatitis B is common. While more long term studies are needed, combining standard vaccination with attention to metabolic health may become an important part of protecting people from this persistent liver virus.
Citation: Adugna, A., Abebaw, D., Ashenef, B. et al. Immunometabolic determinants of hepatitis B vaccine seroprotection among Ethiopian adults. Sci Rep 16, 15310 (2026). https://doi.org/10.1038/s41598-026-47048-x
Keywords: hepatitis B vaccine, cholesterol, inflammation, Ethiopia, healthcare workers