Clear Sky Science · en
Immune mechanisms driving clinical heterogeneity in oral lichen planus
Mouth sores that tell a bigger story
Oral lichen planus is often seen as a stubborn rash inside the mouth, but this study shows it is also a window into how the whole immune system behaves. By comparing people with two common forms of the disease and healthy volunteers, the researchers reveal that seemingly similar mouth spots can be driven by very different immune patterns in the blood.
Two kinds of mouth patches
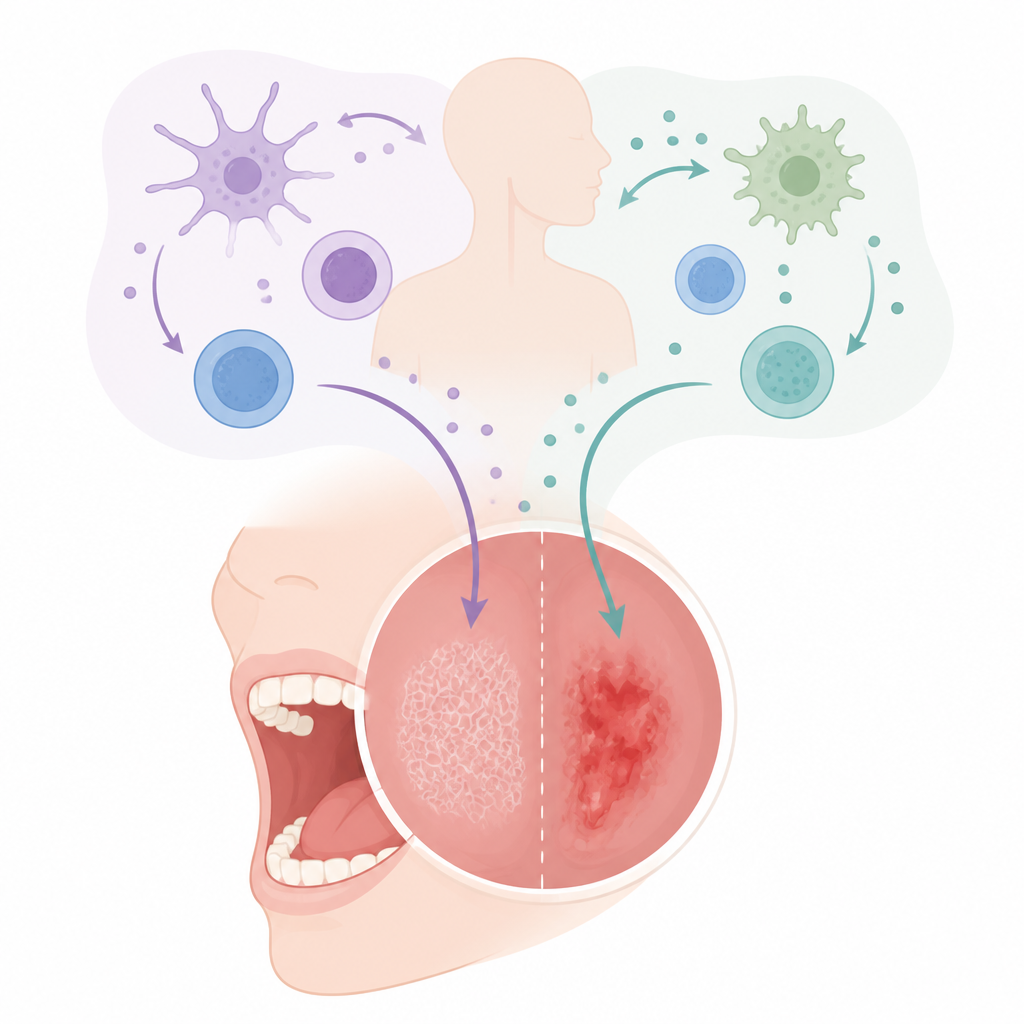
Doctors usually split oral lichen planus into two main types. The reticular form tends to show up as pale, net like streaks on the cheeks and is often mild or symptom free. The erosive form, in contrast, brings raw, painful areas that may bleed and interfere with eating or speaking. Although these changes are limited to the moist lining of the mouth, the team suspected that deeper, body wide immune changes might help explain why some people develop one pattern rather than the other.
Taking a close look at blood cells
The researchers studied blood samples from 61 patients with oral lichen planus and 30 healthy people of similar age and sex. They isolated key white blood cells and used advanced flow cytometry to map many different T cells, B cells, and natural killer cells at once. They then stimulated these cells in the lab to see which chemical messengers, called cytokines, they released. This approach let them compare the internal immune landscape of people with reticular disease, erosive disease, and no disease at all.
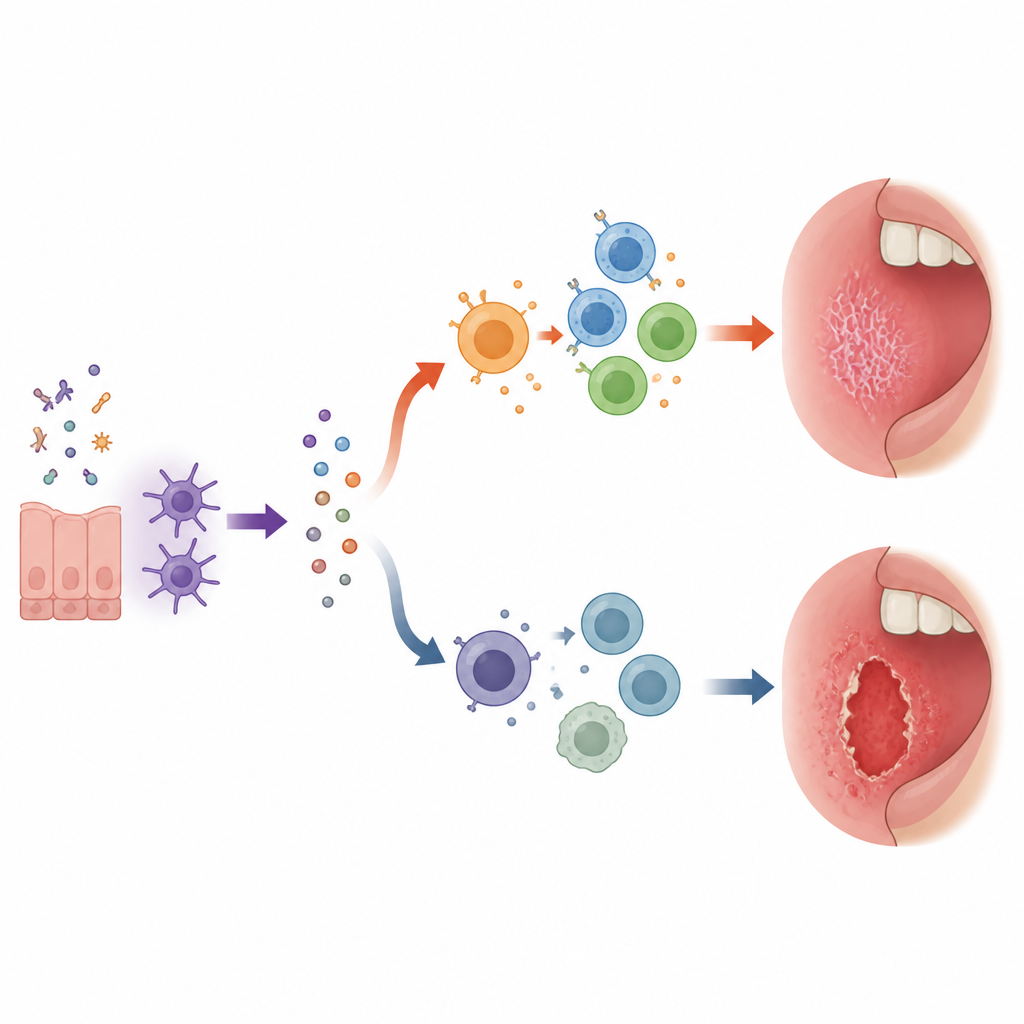
A fiery profile in the milder form
Surprisingly, people with the usually milder reticular form showed the most clearly inflamed profile in their blood. Their stimulated immune cells released higher amounts of several pro inflammatory cytokines, including those linked to T helper type 1 and type 17 responses, which support strong cell killing activity. They also had more T helper type 1 cells among their circulating T cells. At the same time, both patient groups showed an expansion of naive B cells, a type of cell often associated with autoimmunity, and an increase in a subset of B cells that is prone to making self directed antibodies.
A quieter but stubborn signal in the painful form
In the erosive form, the team did not see the same strong burst of inflammatory cytokines. Instead, both forms shared a rise in a calming cytokine called TGF beta 1, with especially persistent levels in erosive disease. Many T cells and natural killer cells in both groups also carried higher amounts of TIGIT, an inhibitory receptor that appears when cells are repeatedly stimulated. Rather than changing the number of these cells, oral lichen planus seems to change how they are tuned, tilting them toward a chronically restrained, possibly exhausted state that may still fail to clear the disease.
What this means for patients
Together, these findings paint oral lichen planus as more than a surface problem. The reticular form is linked to a hot, cytokine driven immune pattern, while the erosive form appears tied to long lasting inhibitory signals and altered B and natural killer cell behavior. For patients, this suggests that different clinical pictures may reflect different underlying immune settings. In the future, carefully targeting these pathways, such as naive B cells or TIGIT related signals, could help doctors move beyond one size fits all treatment and design more tailored approaches to ease symptoms and control this chronic condition.
Citation: Pons-Fuster, E., Conesa-Solano, J., Gimeno-Arias, L. et al. Immune mechanisms driving clinical heterogeneity in oral lichen planus. Sci Rep 16, 15575 (2026). https://doi.org/10.1038/s41598-026-46106-8
Keywords: oral lichen planus, immune system, cytokines, T and B cells, autoimmune inflammation