Clear Sky Science · en
Multimodal contrastive prognostication framework for early neurological outcome prediction in post-cardiac arrest patients
Why early brain outcome after cardiac arrest matters
After a sudden cardiac arrest, many people are resuscitated but remain unconscious, leaving families and clinicians in painful uncertainty about whether the brain will recover. Current guidelines often delay firm predictions for three days or more, even though critical decisions about treatment intensity, resource use, and family expectations must be made much sooner. This study explores whether artificial intelligence can safely use information already available in the first hours after resuscitation to give clearer, earlier insight into likely brain recovery.
A closer look at the problem
Sudden cardiac arrest affects hundreds of thousands of people each year in the United States, with survival and meaningful brain recovery remaining rare. After blood flow is restored, many patients stay in a coma because of oxygen deprivation to the brain. Doctors can examine pupils and movements, look at brain waves, measure blood markers, and review brain scans, but each of these tools on its own is imperfect. Sedation, equipment limitations, and conflicting test results all contribute to uncertainty. Because of these challenges, many hospitals wait at least 72 hours before offering a firm prognosis, leaving a gap in the early period when the course of care is being set.
A new way to combine scans and bedside data
To address this gap, the researchers built a multimodal AI system called CLAIR that blends brain CT scans with routine clinical information to predict a patient’s Cerebral Performance Category score, a standard measure of brain outcome at hospital discharge. CLAIR does not just look at a single image or a single number. Instead, it takes in CT reconstructions from three views of the head along with data such as age, time until the heart started beating again, body temperature, lab markers, and results from electrical brain tests when available. A specialized architecture allows the model to let the image features and clinical features “pay attention” to each other, so that the meaning of a scan can be interpreted in the full clinical context. 
How the study tested the model
The team retrospectively analyzed 208 adults who had cardiac arrest and at least one head CT at a single medical center between 2020 and 2022. Patients who had life support withdrawn for non-brain reasons were excluded to focus on neurological outcomes. Overall, 306 CT scans were collected, but crucially, the main tests of CLAIR used only scans obtained within the first 24 hours after the arrest, with a median timing of just over three hours. The data were split by patient into training, validation, and test sets to avoid any overlap. CLAIR was trained and evaluated in two versions: one using only information available early after admission, and another that also included later test results gathered over the hospital stay.
How well CLAIR performed
CLAIR’s predictions were compared with those of a strong imaging-only deep learning model and with assessments by two experienced neurologists. When fed both multi-view CT scans and early clinical data, CLAIR achieved an area under the ROC curve of 0.94, clearly higher than the CT-based imaging-only approach, which reached about 0.80. This means CLAIR was better at distinguishing patients who would eventually have good brain function from those who would not. Both versions of CLAIR showed high accuracy, sensitivity, and specificity. In a separate exercise on 20 especially challenging cases, each human and AI evaluator made some mistakes, but clinicians who were allowed to see CLAIR’s predictions made fewer prognostic errors than when working alone, suggesting that the tool can act as a useful second opinion rather than a replacement for expert judgment. 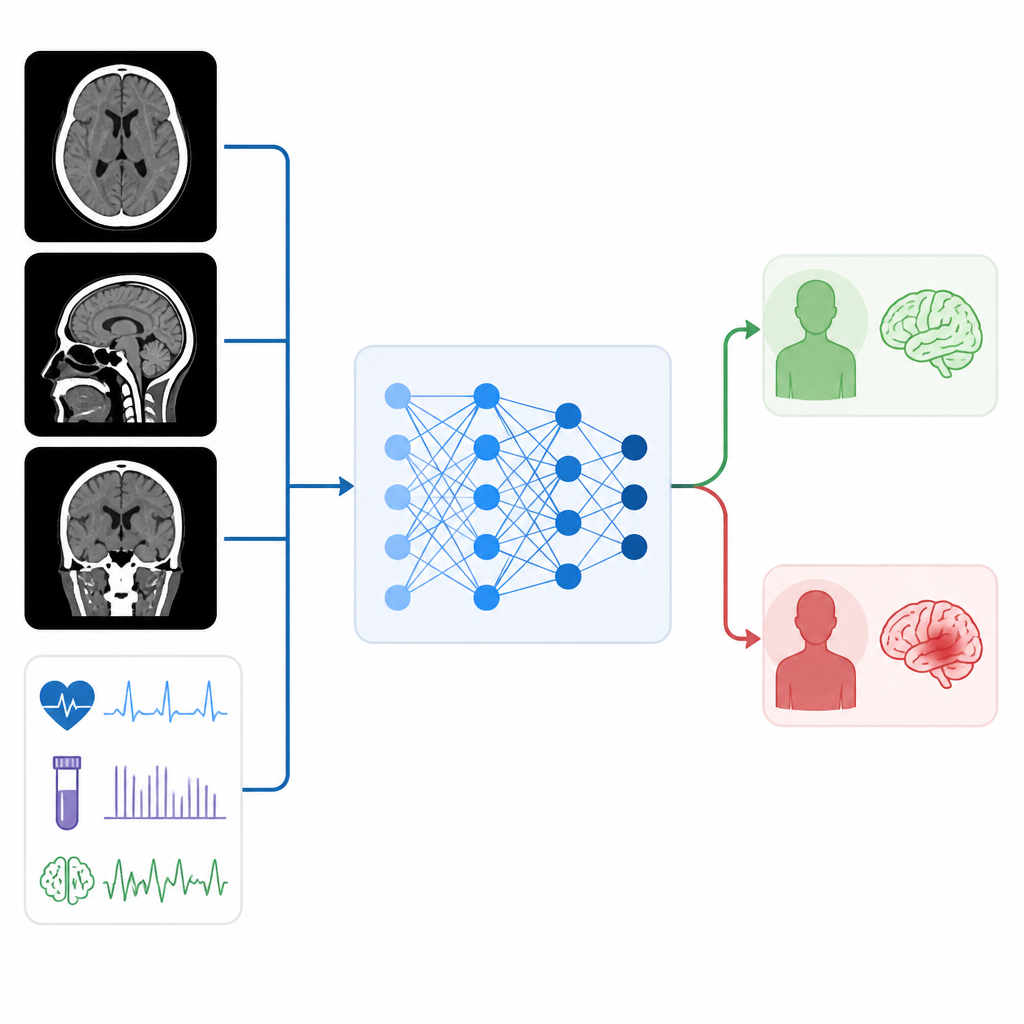
What this could mean for patients and families
The study shows that an AI system that jointly analyzes early brain CT scans and bedside clinical data can provide more accurate early forecasts of neurological outcome after cardiac arrest than imaging-only methods. While the work is based on a single-center, modest-sized dataset and needs confirmation in larger, more diverse populations, it points toward a future in which doctors and families may not have to wait days for a well-informed picture of likely recovery. Used carefully alongside clinical expertise, such tools could support more timely and thoughtful decisions about ongoing treatment, communication with loved ones, and the fair use of intensive care resources.
Citation: Kasturi, A., Proctor, A.R., Vosoughi, A. et al. Multimodal contrastive prognostication framework for early neurological outcome prediction in post-cardiac arrest patients. Sci Rep 16, 15582 (2026). https://doi.org/10.1038/s41598-026-45573-3
Keywords: cardiac arrest, neurological outcome, brain CT, artificial intelligence, prognostication