Clear Sky Science · en
Finite element analysis of sacral fixation strategies for fragility fractures of the pelvis
Why weak bones in the pelvis matter
As people live longer, more older adults suffer small but serious breaks in the bones of the pelvis, often after a minor fall. These “fragility” fractures can make even simple movements unbearably painful, confine people to bed, and trigger complications such as pneumonia or blood clots. Surgeons now use minimally invasive screws and rods to stabilize these fragile bones, but they still debate which screw patterns are safest and strongest, especially in thin, brittle bone. This study used computer modeling to test several screw layouts in a virtual pelvis, aiming to find which approach best supports healing while limiting the risk of hardware failure.
How the pelvis can quietly break
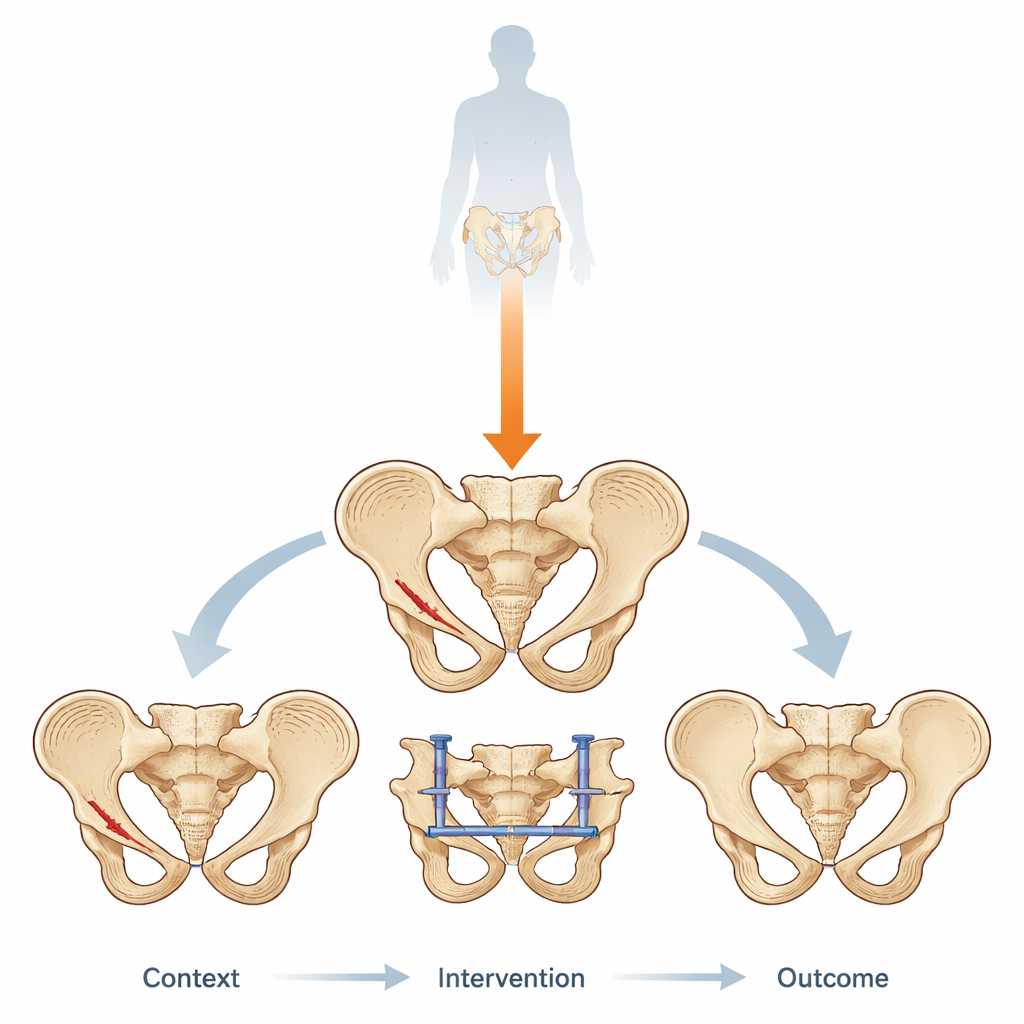
The pelvis forms a ring of bone that carries the weight of the upper body into the legs. In older adults with osteoporosis, this ring can crack in the front and back after a low-energy fall or even routine activity. The authors focused on a common pattern: a break in the pubic bone at the front and a fracture in the sacrum at the back, near where the spine meets the pelvis. These injuries are tricky, because surgeons must stabilize both the front and back of the ring to allow safe early walking, yet the bone itself is fragile and less able to grip screws. Choosing the wrong fixation layout can lead to painful motion at the fracture, loosening of screws, and the need for repeat surgery.
A virtual pelvis put to the test
To explore these trade-offs safely, the researchers built a detailed three-dimensional computer model of the pelvis of a 65-year-old woman, based on CT scan data. They digitally “broke” the bone in a typical fragility pattern and then added a standard front-side device called an INFIX, a bar that runs under the skin to stabilize the front of the ring. On the back, they tested six different screw layouts crossing the sacrum and the joints between the sacrum and hip bones. These layouts differed in two main ways: whether screws were placed at one level (either the upper sacral segment S1 or the lower segment S2) or at both levels together, and whether the screws were short, ending in one pelvic bone, or long, running all the way across from one side of the pelvis to the other.
What the computer revealed about stress and motion
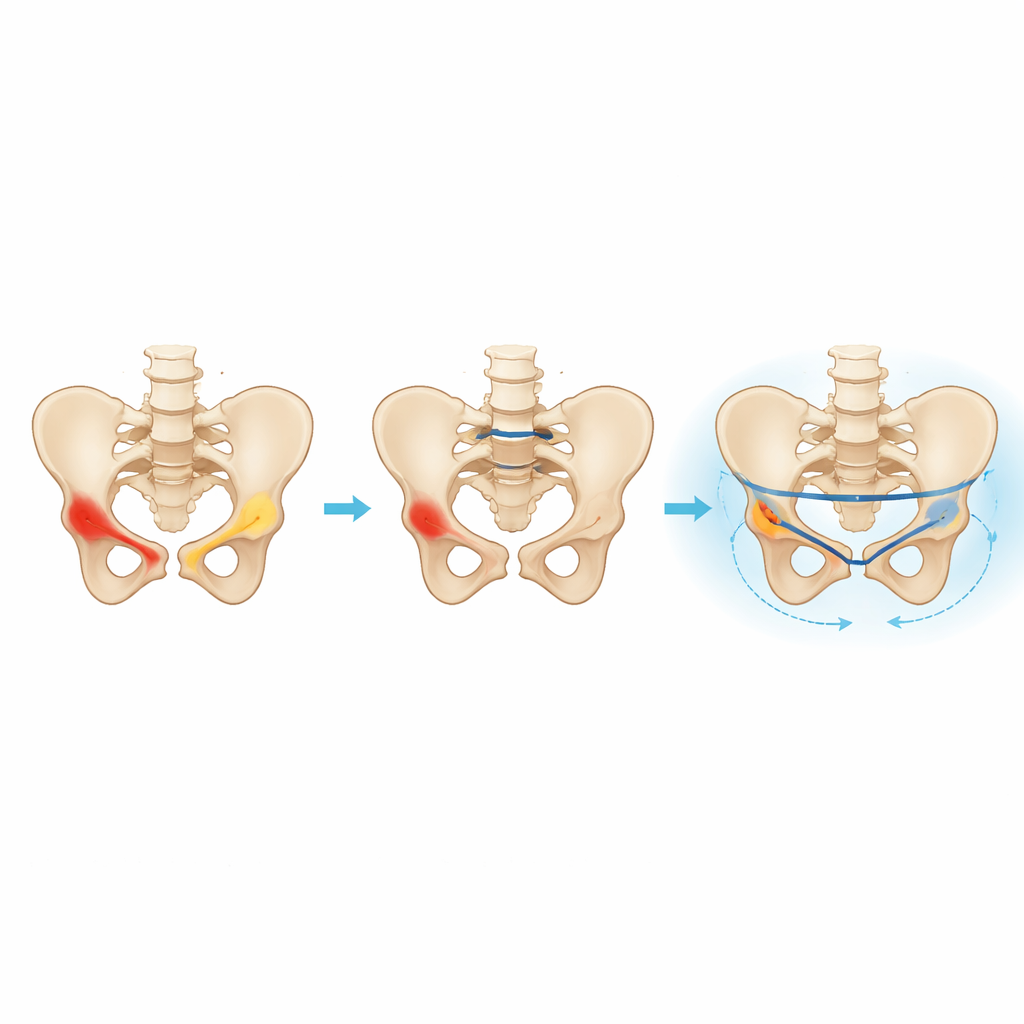
The team then “loaded” the model by pushing down on the top of the sacrum with a force similar to body weight while the hip sockets were held in place, mimicking standing. They tracked how much the fractures opened or shifted and how much mechanical stress built up in the screws and along the fracture lines. The front-side INFIX bar performed well in all cases, with very small movement at the pubic fracture and low internal stress, meaning it was unlikely to fail under these conditions. The real differences appeared in the back of the pelvis. Constructs that used screws at both S1 and S2 showed less motion at the sacral fracture and distributed stress more evenly than those with a single screw level. Among all options, the layout using two long screws that crossed the sacrum at both levels produced the smallest fracture movement and a favorable pattern of stress sharing between bone and hardware, even though the screws themselves carried somewhat higher loads.
Balancing stability and hardware demands
The step-by-step stress maps of the bone and screws highlighted a key idea: using two levels of fixation helps spread forces across the back of the pelvis, reducing concentrated stress at the fracture surface and at any one screw. Long screws that run from one hip bone, through the sacrum, and into the opposite side further improve load sharing, especially when used at both sacral levels. However, this added stiffness comes with a trade-off: the long screws themselves see higher stress and may be technically harder and riskier to insert in real patients because of nearby nerves, blood vessels, and narrow bone corridors. The model also confirmed that all stresses stayed below the strength of the titanium material, so the differences reflect relative safety margins rather than imminent breakage.
What this means for patients and surgeons
Translated into everyday terms, the study suggests that, for older adults with fragile pelvic fractures, stabilizing the back of the pelvis with screws at two levels, and using long screws that cross the sacrum when anatomy allows, can create a more stable “frame” for healing and early movement. When such long screws cannot be safely placed, combinations of screws at both levels using shorter implants still offer acceptable mechanical support. The work does not replace clinical trials, but it provides a physics-based map of how different screw patterns share the load, helping surgeons tailor safer, more reliable minimally invasive repairs for some of the most vulnerable patients.
Citation: Liu, S., Zhang, L., Xue, C. et al. Finite element analysis of sacral fixation strategies for fragility fractures of the pelvis. Sci Rep 16, 14318 (2026). https://doi.org/10.1038/s41598-026-45149-1
Keywords: pelvic fragility fractures, sacroiliac screw fixation, osteoporosis, finite element analysis, minimally invasive surgery