Clear Sky Science · en
Immunogenomic classification reveals prognostic immune signatures in pediatric solid and hematological tumors
Why the Body’s Defenses Matter in Childhood Cancer
Parents of children with cancer often hear about chemotherapy, surgery and radiation, but far less is said about the body’s own defense system. This study asks a simple question with big implications: can patterns in a child’s immune system help predict how well they will do, and point to new treatment ideas? By reading the genetic activity of tumors from many young patients, the researchers map how immune cells surround and interact with cancers, and show that these patterns are linked to survival in several common pediatric tumors.
Taking a Wide Look at Childhood Tumors
The team examined data from more than 2,700 childhood cancers stored in large public and hospital databases. These included solid tumors such as neuroblastoma, osteosarcoma, Wilms tumor, rhabdoid tumor and clear cell sarcoma of the kidney, as well as blood cancers like acute myeloid leukemia and acute lymphoblastic leukemia. Instead of looking at single genes, they focused on groups of genes that reflect the presence and activity of different immune cells, such as T cells, B cells, natural killer cells, neutrophils and others that either fight or support tumors. Using these immune “signatures,” they grouped solid tumors into five immune types and blood cancers into four, each with its own typical mix of immune activity.
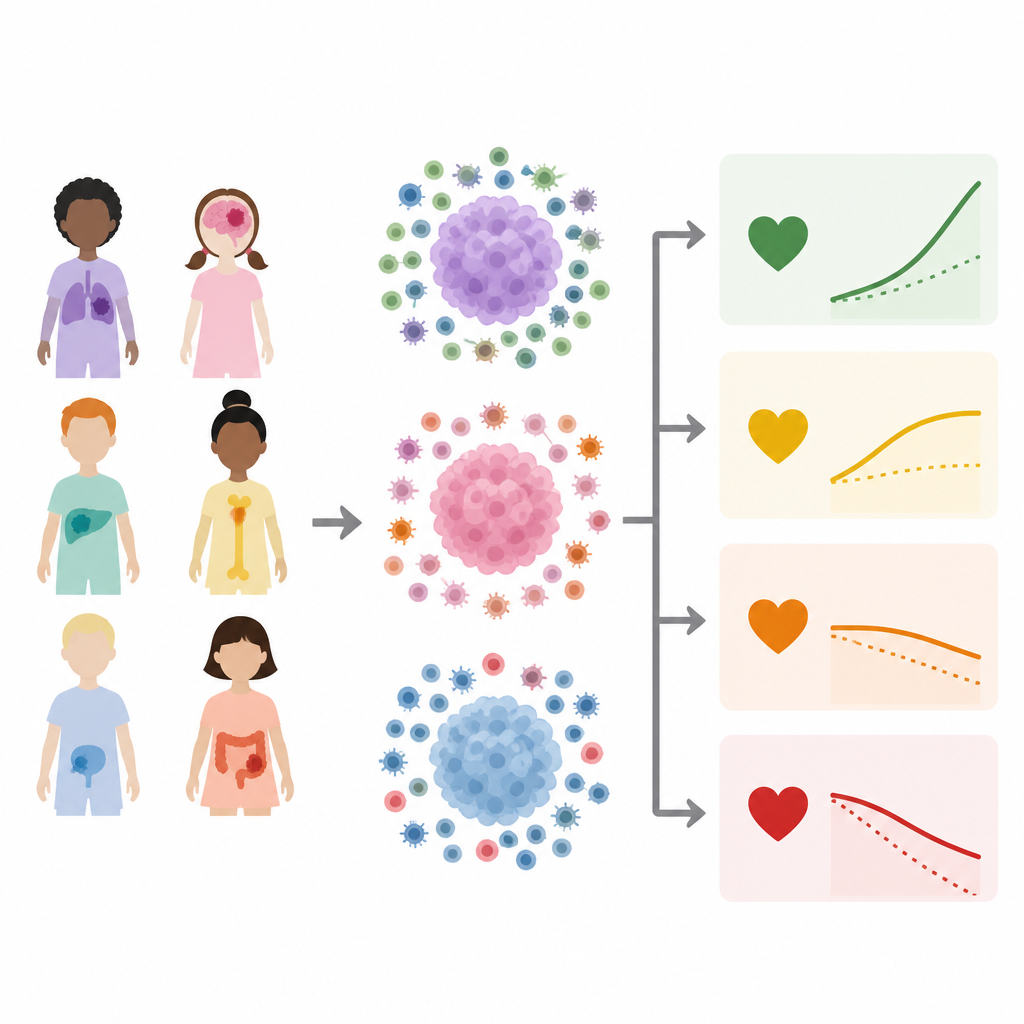
Good and Bad Immune Patterns in Solid Tumors
For pediatric solid tumors, the five immune types showed strikingly different outcomes. One group, called S1, showed strong signals of wound healing and active B cells, a pattern that matched the poorest overall survival. In contrast, another group, S4, had much lower levels of these features and higher activity from cells and pathways related to blood vessel growth, natural killer cells and neutrophils. Children whose tumors fell into the S4 group generally lived longer. The team confirmed this pattern in an independent set of neuroblastoma patients from a children’s hospital, where tumors with S4-like gene activity again tracked with better survival, suggesting that this immune pattern is robust and clinically meaningful.
Immune Landscape in Childhood Blood Cancers
In blood cancers, the picture was more complex. The four immune types reflected different mixes of monocytes, neutrophils, antigen processing activity and T cell signals. One type, H4, generally showed lower levels of many immune features but relatively higher T cell signals and was tied to better survival across the full group of pediatric blood cancers. However, when the researchers zoomed in on acute myeloid leukemia, they found that the same immune type could mean different things depending on a key genetic change called FLT3-ITD. In FLT3-ITD positive leukemia, an immune pattern rich in neutrophils and monocytes was linked to the worst survival, while in FLT3-ITD negative cases the very same pattern was associated with better outcomes. This shows that tumor genetics and immune context must be considered together.
Finding Gene Clues and a Score for Neuroblastoma
To better understand what drives these patterns, the researchers searched for immune-related genes and pathways that were more active in specific immune types and also linked to survival. In solid tumors, they highlighted genes tied to blood vessel growth, neutrophils and certain B cell functions. In blood cancers, they found genes connected to monocytes, natural killer cells, TGF beta signaling and T cells. For neuroblastoma, they distilled 44 genes that were especially active in the favorable S4 immune type and associated with longer survival. They combined these into an “S4 gene score” that could be calculated for each tumor sample. Children with high S4 scores in both the public dataset and the hospital cohort tended to live longer, suggesting this simple score could help doctors estimate risk using a single test.
What This Means for Children and Their Care
This work shows that the immune surroundings of a tumor are not just background noise but hold important clues about a child’s outlook. Certain mixes of immune cells and signals go hand in hand with better or worse survival, and these patterns can differ even within the same cancer type depending on genetic mutations. While more research and clinical testing are needed, immune-based groupings and scores like the S4 gene score could eventually help doctors tailor treatments, select patients for immunotherapies and design smarter clinical trials. For families, the message is that understanding and harnessing a child’s own defenses may become an important part of future cancer care.
Citation: Xia, Z., Hua, Q., Qian, J. et al. Immunogenomic classification reveals prognostic immune signatures in pediatric solid and hematological tumors. Sci Rep 16, 15554 (2026). https://doi.org/10.1038/s41598-026-44997-1
Keywords: pediatric cancer, tumor immune microenvironment, neuroblastoma, acute myeloid leukemia, immunogenomics