Clear Sky Science · en
Modeling optimal timing of immunotherapy and chemotherapy to prevent resistance and recurrence in triple-negative breast cancer
Why timing of cancer treatment matters
Many people know that triple negative breast cancer is one of the most aggressive forms of breast cancer, but fewer realize that when drugs are given can be as important as which drugs are chosen. This study uses mathematics and laboratory data to explore how carefully timed combinations of chemotherapy and immunotherapy might keep this cancer from coming back by outsmarting both the tumor and its interactions with the immune system.
How a shape-shifting tumor evades attack
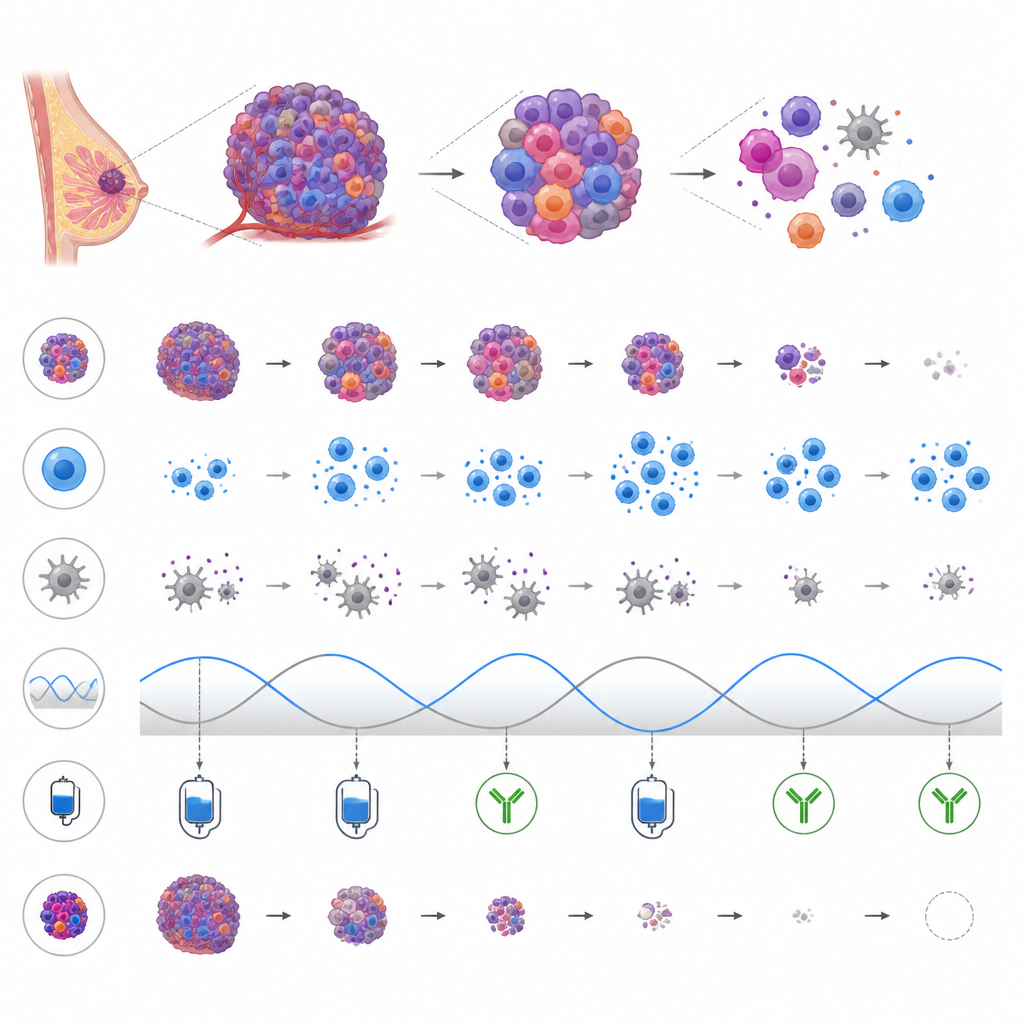
Triple negative breast cancer lacks three common hormone related markers, which makes it harder to target with standard drugs. The tumor is also highly flexible: its cells can switch between different states, some more stem cell like and therapy resistant than others. In mice, one surface marker called Sca 1 helps distinguish these states. On top of this, the immune system is both friend and foe. Killer cells such as natural killer cells and T cells can destroy cancer cells, while myeloid derived suppressor cells act as bodyguards for the tumor by dampening immune attacks. This shifting balance between cancer cells and various immune cells sets the stage for either cure, quiet dormancy, or uncontrolled growth.
Building a virtual tumor and immune system
To untangle this complex dance, the researchers built a computer model using ordinary differential equations, a common mathematical tool for tracking how populations change over time. They fed the model with experimental measurements from mouse triple negative breast cancer cells and immune cells. The model follows several tumor cell groups, including drug sensitive cells, more plastic Sca 1 positive cells, and a chemotherapy selected resistant group, along with immune killer cells and suppressor cells. It also includes two treatments: methotrexate, a long used chemotherapy drug that kills rapidly dividing cells but can weaken blood cell production, and Abequolixron (RGX 104), an experimental drug that reduces suppressor cells and boosts anti tumor immunity.
Testing treatment plans inside the computer
With this virtual system, the team could safely run thousands of treatment scenarios that would be impossible to test in living animals. They varied when treatment began, how long methotrexate remained active, how long drug free breaks lasted, and whether the immune boosting drug was added. For each scenario, the model classified the long term outcome as tumor elimination, escape, or a dormant state with a stable but nonzero number of cancer cells. The simulations showed rich oscillations in immune and tumor cell numbers over time, reflecting feedback between tumor growth, immune activation, and immune suppression.
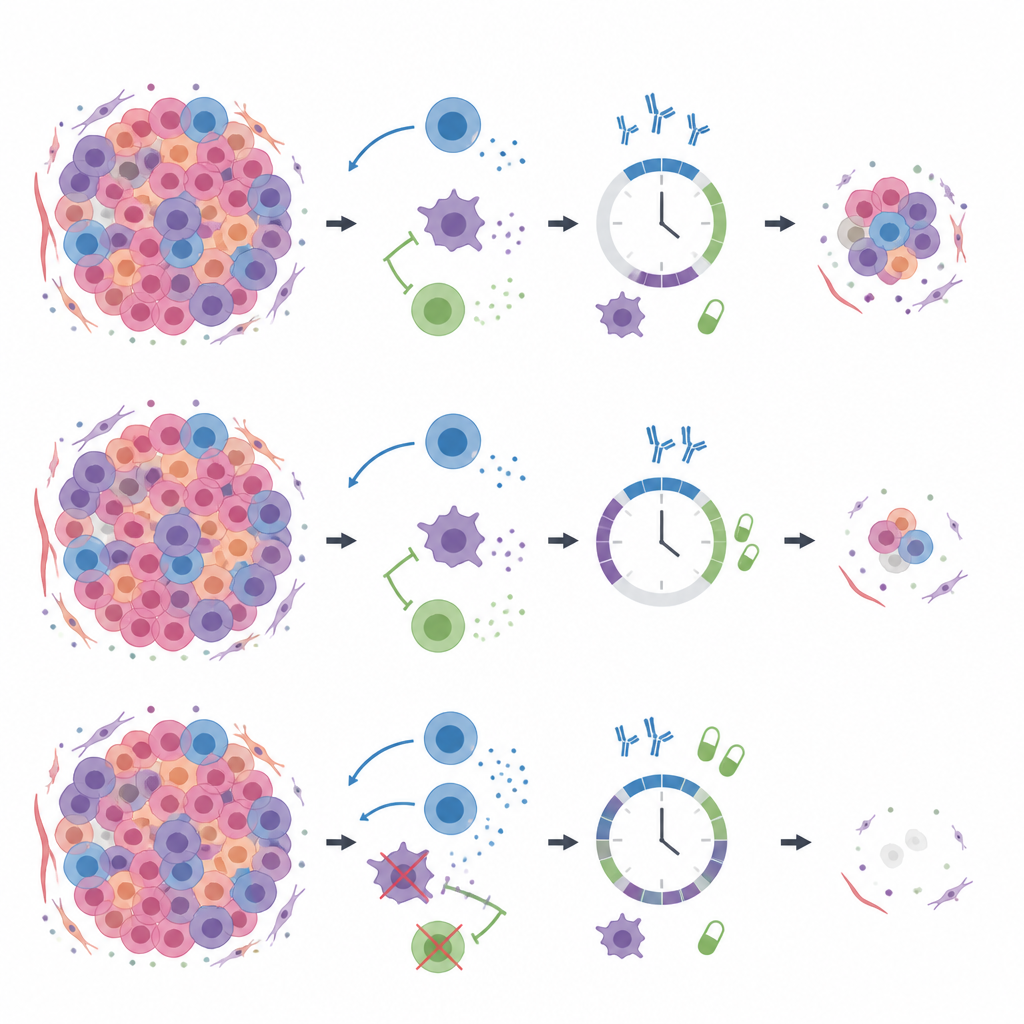
What makes a schedule succeed or fail
The analysis revealed that timing is crucial. Starting chemotherapy when immune killer cells are near a natural peak made elimination far more likely, because the drugs cut down the tumor just as the immune system is poised to strike. If treatment began too early or too late in this immune cycle, the tumor tended to escape. Chemotherapy also had to be given for a “just right” duration. Very short courses left mainly drug sensitive cells that could regrow, while prolonged exposure favored the rise of resistant cells that then drove relapse. Surprisingly, longer rests between methotrexate cycles often pushed tumors from dormancy toward elimination by allowing immune recovery without giving resistant cells a strong competitive edge. Adding the immune boosting drug before or together with chemotherapy widened the range of schedules that worked, especially when the natural killing power of immune cells was modest.
What this could mean for patients
In simple terms, the study suggests that triple negative breast cancer may be better controlled not only by combining chemotherapy and immunotherapy, but by giving them in the right order and at the right moments in the immune cycle. A short, well timed dose of chemotherapy, flanked by periods that let the immune system rebound and by drugs that remove immune suppressor cells, can shrink the tumor and prevent resistant cells from taking over. While this work is based on mouse data and computer simulations rather than direct patient trials, it offers a quantitative roadmap for designing treatment schedules that aim to avoid both resistance and silent dormancy, potentially lowering the risk of cancer returning.
Citation: Daneshparvar, M., Ghanizadeh, M., Shariatpanahi, S.P. et al. Modeling optimal timing of immunotherapy and chemotherapy to prevent resistance and recurrence in triple-negative breast cancer. Sci Rep 16, 15450 (2026). https://doi.org/10.1038/s41598-026-44611-4
Keywords: triple negative breast cancer, chemo immunotherapy, treatment timing, drug resistance, mathematical modeling