Clear Sky Science · en
72-hour SOFA changes and risk stratification for invasive mechanical ventilation in patients with community-acquired Pneumonia
Why this hospital study matters
When someone is admitted to the hospital with pneumonia caught in the community, one of the most urgent questions for doctors and families is whether that person will end up needing a breathing machine. This decision has huge consequences: it affects survival, time in the intensive care unit, and how hospital resources are used. The study behind this article asks whether watching how a patient’s organs respond over the first three days in the hospital can give a clearer early warning than traditional one‑time scores taken on the day of admission.
From first snapshot to moving picture
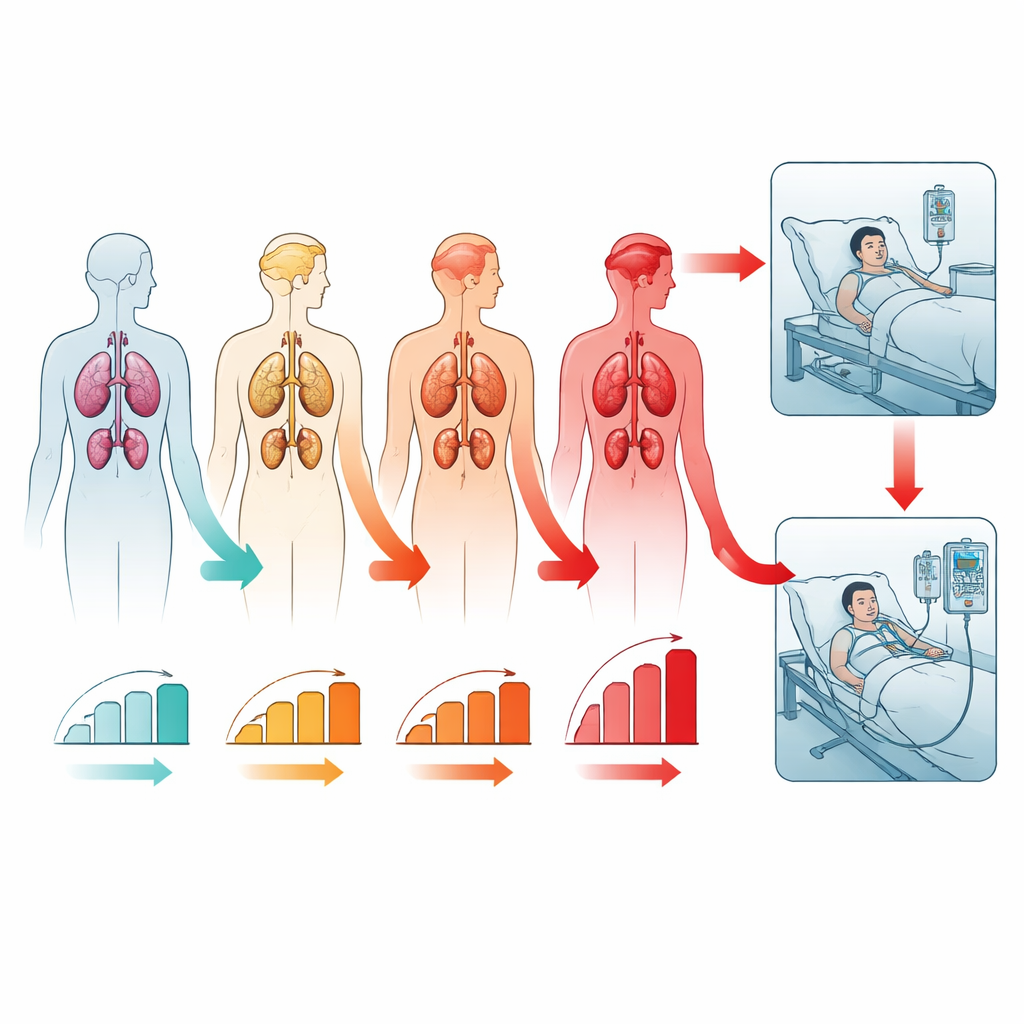
Today, doctors usually judge pneumonia severity using scores such as PSI or CURB‑65, which combine age, vital signs, and lab tests into a single number. These tools work reasonably well for predicting who might die, but they are based on a single snapshot taken at admission. They say little about how a patient is actually responding to treatment after a couple of days. In contrast, the SOFA score tracks the function of six major organ systems, from lungs to kidneys to brain, and can be repeated over time. The researchers wondered whether changes in this organ score over the first 72 hours could turn that one‑time snapshot into a moving picture that better predicts who will need invasive mechanical ventilation, where a tube is placed into the windpipe and a machine takes over breathing.
A simple A–B–C–D way to group patients
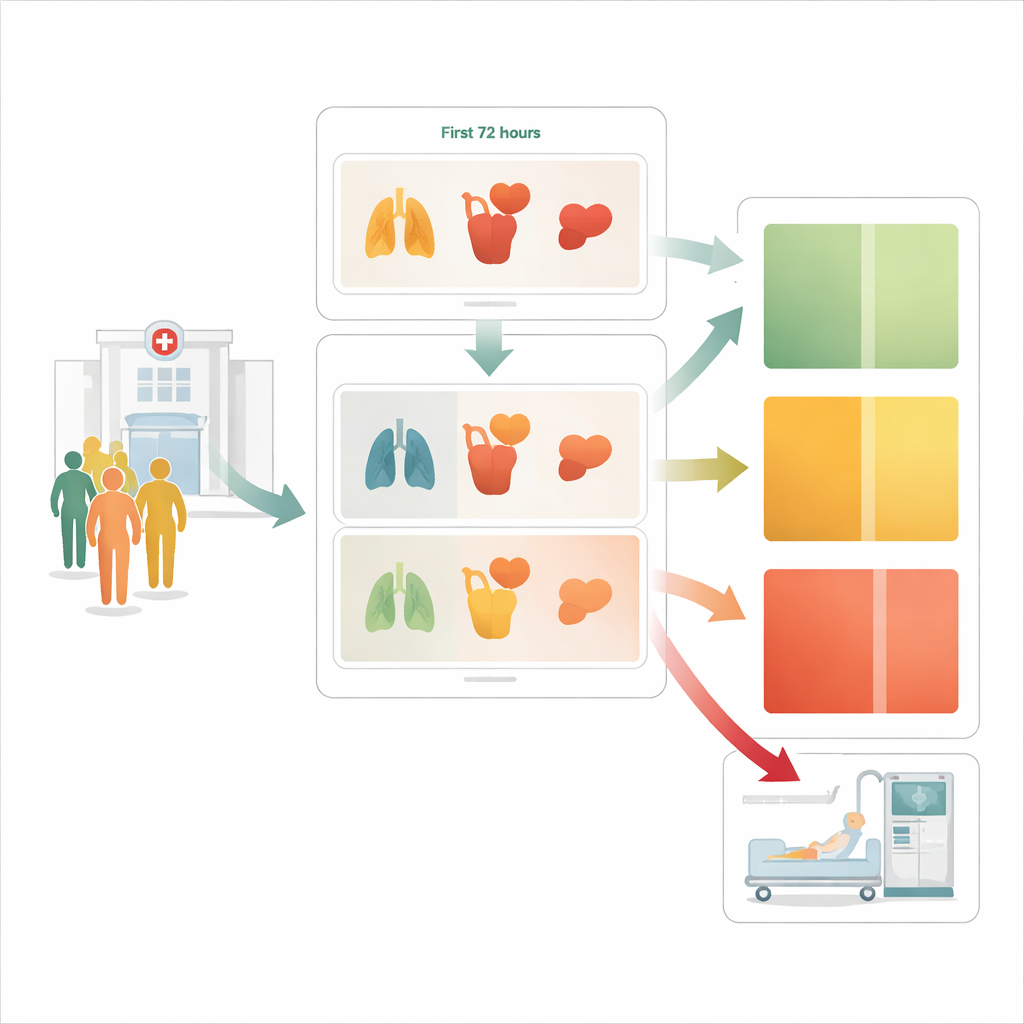
The team analyzed data from 581 adults hospitalized with community‑acquired pneumonia in a Colombian hospital. Every patient had a SOFA score measured on admission and again about 72 hours later. The researchers then built a simple two‑by‑two grid. First, they split patients into “low” versus “high” risk at admission based on their initial SOFA score. Second, they checked whether the score stayed the same or improved, or instead worsened over the first three days. This created four easy‑to‑remember groups: low‑risk patients who stayed stable, low‑risk patients who deteriorated, high‑risk patients who stabilized, and high‑risk patients who continued to worsen.
Four paths, four very different chances of a breathing machine
The four groups had strikingly different chances of ending up on a ventilator. Among low‑risk patients whose organ function stayed stable or improved, only about 1 in 20 needed invasive ventilation. But if those same low‑risk patients’ organ scores worsened over 72 hours, the chance jumped to about 1 in 3. High‑risk patients who stabilized also had about a 30% chance of ventilation, while those who started off high‑risk and then deteriorated further were in a very dangerous zone: more than 4 out of 5 eventually needed a breathing machine. In statistical models that accounted for standard pneumonia scores, simply knowing whether the SOFA score worsened within 72 hours multiplied the odds of ventilation almost fourteen‑fold.
Building a better early‑warning calculator
To test how useful this information could be, the researchers compared two prediction tools. The first used only traditional admission‑day measures, such as PSI, CURB‑65, and whether a patient’s initial SOFA score was low or high. The second “dynamic” tool added one extra ingredient: did the SOFA score worsen over 72 hours or not? The dynamic model clearly performed better. It was more accurate at telling apart patients who would and would not need invasive ventilation, reclassified many people into more appropriate risk categories, and offered a higher overall “net benefit” when the authors simulated real‑world decision‑making. Using an optimal cutoff from the dynamic model, doctors could flag about one‑third of patients as high risk, correctly catching roughly two‑thirds of those who would go on to need a breathing machine while keeping the rate of false alarms relatively low.
What this means for patients and care teams
For patients with pneumonia who remain in the hospital for at least three days, this study suggests that how their organs behave over those first 72 hours matters as much as, or more than, how sick they look when they arrive. A simple framework that combines starting organ status with early change can sort people into clearly different risk groups and sharpen doctors’ judgment about who may soon need intensive breathing support. While the work comes from a single center and still needs to be confirmed in other hospitals and countries, it points toward a more dynamic style of risk assessment: not just “How sick is this person now?” but “Which way are they heading?” That shift could help clinicians target closer monitoring and preparations for ventilation to those most likely to need it, while avoiding unnecessary worry and interventions for those on a safer path.
Citation: Liu, G., Ou, J., Yang, T. et al. 72-hour SOFA changes and risk stratification for invasive mechanical ventilation in patients with community-acquired Pneumonia. Sci Rep 16, 13815 (2026). https://doi.org/10.1038/s41598-026-44586-2
Keywords: community-acquired pneumonia, mechanical ventilation, organ failure score, hospital risk assessment, critical care