Clear Sky Science · en
Multi-constraint calibrated GP2SFCA identifies dual vulnerability in private-vehicle access to Tertiary Grade‑A emergency care of Chengdu
Why reaching care in time matters
When a medical emergency strikes, minutes can mean the difference between life and death. In fast-growing megacities like Chengdu, people often rely on private cars to reach top-tier hospitals, yet heavy traffic and unevenly placed facilities can silently decide who gets timely help. This study asks a simple but pressing question: how fairly is emergency care by car distributed across the city, and how do everyday traffic patterns and human choices shape that access?

A city with hospitals in the middle
Chengdu’s best hospitals are tightly clustered in the central urban districts, while many suburban and rural residents live far away from this medical core. The researchers built a detailed picture of the city using census population data, official hospital statistics, road maps and real-time driving times from a popular navigation service. Instead of assuming that roads are always clear or that distance is the same as time, they used live travel times that change by hour and by day, capturing how congestion really affects a rushed trip to the emergency department.
Following real journeys instead of simple distance
To move beyond older, static models of access, the team created a new framework called GP2SFCA that mimics how people actually choose a hospital under pressure. First, it filters out hospitals that are simply too far to reach within a set time window such as 30, 10 or 5 minutes of driving. Then, among the remaining options, it treats hospital choice as a probability rather than assuming everyone always goes to the single closest site. This two-step view allows the model to distinguish between places that are cut off because nothing is reachable in time and places where several hospitals compete for the same pool of patients.
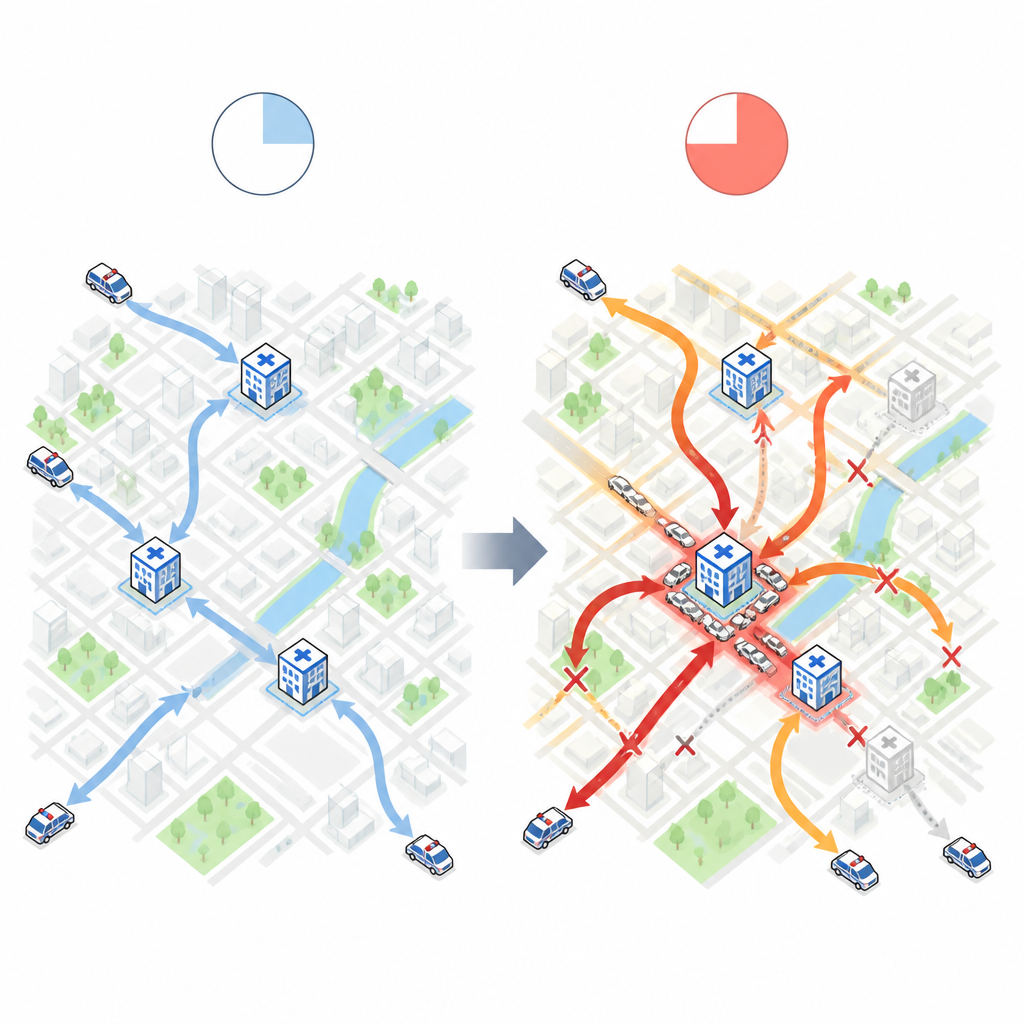
What traffic and time windows reveal
By running this model across three time limits and six traffic situations, the study uncovered a striking pattern of “dual vulnerability.” During weekday rush hours, especially with a 10-minute limit, accessibility collapses in the suburbs as commuting traffic slows cars and shrinks the set of hospitals that can be reached. This regular, predictable weakness reflects how tidal flows of workers overload key corridors. On weekends, when commuting eases, access improves somewhat on the outskirts, but new pockets of poor access appear inside the city center, near famous hospitals whose popularity and leisure-time traffic combine to create local bottlenecks.
How urgency sharpens our choices
The researchers also measured how strongly people’s choices respond to extra minutes of travel as the clock ticks down. They estimated a key number that describes how quickly access falls off with travel time, and found that it rises steadily as the time window tightens: from under 1 for a 30-minute drive to well above 2 for a 5-minute dash. In everyday terms, the more urgent the situation and the heavier the congestion, the more people favor very nearby hospitals and the more sharply access drops for those living even a little farther away. This pattern held up under many tests, suggesting it reflects a real behavioral tendency rather than an artifact of the model.
What this means for city planning
For non-specialists, the main lesson is that emergency access is not fixed by the number of hospitals alone. It emerges from the interplay between where hospitals are built, how traffic ebbs and flows, and how people adjust their decisions under stress. Chengdu’s experience shows that a city can have many high-level hospitals yet still leave large areas exposed at critical moments. Tools like the GP2SFCA framework can help planners see where structural gaps, rush-hour slowdowns and weekend crowding combine to put residents at risk, guiding smarter decisions on new facilities, traffic management and local road design so that more people can reach life-saving care in time.
Citation: Luo, C., Liu, C., Ma, T. et al. Multi-constraint calibrated GP2SFCA identifies dual vulnerability in private-vehicle access to Tertiary Grade‑A emergency care of Chengdu. Sci Rep 16, 15095 (2026). https://doi.org/10.1038/s41598-026-44434-3
Keywords: emergency care access, urban traffic, hospital accessibility, Chengdu megacity, health equity