Clear Sky Science · en
Quantitative analysis of gaze and body movement differences by proficiency in direct and video laryngoscope intubation
Why how doctors look and move matters
When a patient cannot breathe on their own, doctors must quickly place a breathing tube into the windpipe. This high‑stakes procedure, called tracheal intubation, is usually taught through hands‑on practice and expert tips rather than hard numbers. The study behind this article asks a simple question with life‑or‑death implications: how do the eyes and body of an experienced doctor behave differently from those of a beginner, and can new tools help novices mimic expert habits more quickly?
Watching the eyes and body during a vital procedure
To explore this, the researchers turned a training room into a mini motion‑capture studio. Fifteen anesthesiology staff members, seven highly experienced and eight relatively new to intubation, practiced placing breathing tubes into a realistic medical mannequin. Reflective markers on their heads, trunks, arms, and waist recorded how they moved, while special glasses tracked where they looked in three‑dimensional space. This approach allowed the team to measure, frame by frame, how participants positioned their heads and where their gaze fell as they guided the tube into the airway.
Two tools, two ways of seeing the airway
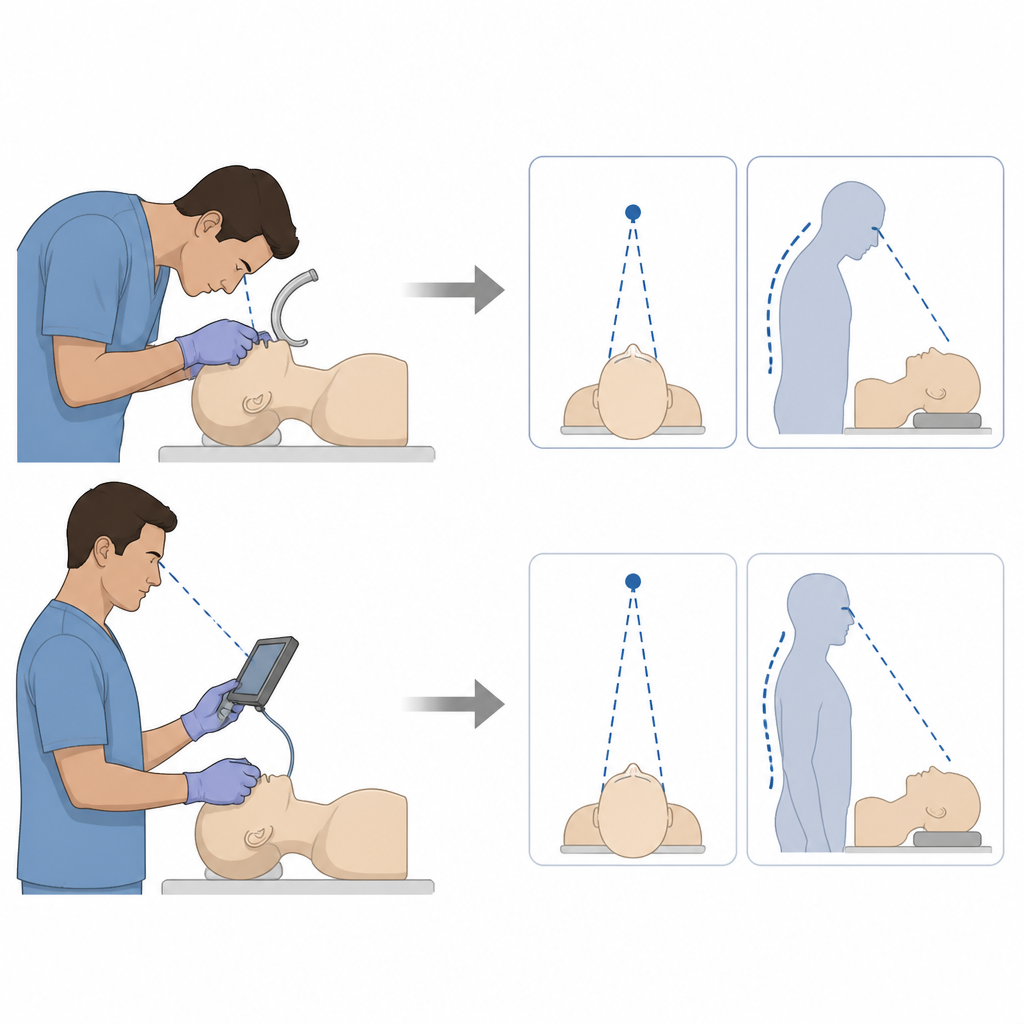
The team compared two common instruments. A traditional direct laryngoscope requires the operator to look straight into the mouth to see the opening of the windpipe. A video laryngoscope carries a tiny camera near its tip, showing the same region on a monitor. Both devices can save lives, but educators have noticed that trainees often succeed more easily with the video version. The new study asks why, in terms of eye position and body posture, this might be the case. By splitting the procedure into phases, especially the moment when the scope is guided into place and when the tube is advanced, the researchers could see how the tools subtly changed behavior.
How experts see the big picture
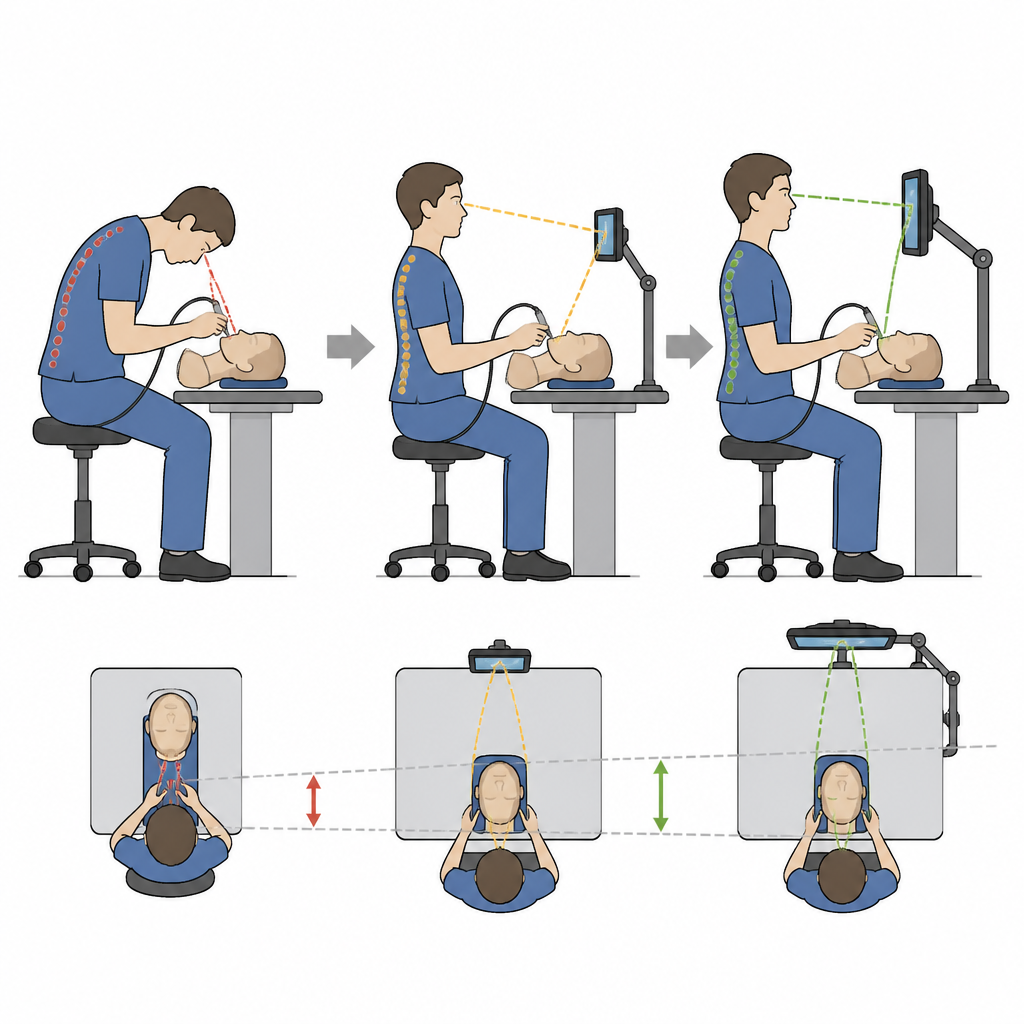
With the direct laryngoscope, clear differences emerged between seasoned clinicians and novices. Experts kept their heads farther from the mannequin’s mouth and their gaze directed slightly beyond their hands, giving them a broader view of the throat region. Their head paths were smooth and nearly straight, suggesting a stable, confident posture. Novices, in contrast, tended to lean forward and down, bringing their faces close to the mouth and focusing on their own hands and the nearby tissue. Their head paths curved downward, and their gaze fell at shorter distances, hinting at a narrower, more tentative field of view. Statistical tests confirmed that experts maintained significantly greater head‑to‑mouth distance and longer gaze distance in key parts of the procedure.
How video tools help beginners act like experts
When participants switched to the video laryngoscope, the gap between experts and novices shrank. Both groups could rely on the screen for visual information, so they no longer needed to lean deeply into the mannequin’s face. Head movement became smaller and more upright, and the differences in gaze distance largely disappeared during the phases when instruments were in motion. Novices in particular kept their heads farther back compared with when they used the direct tool, and their pattern of eye movements became closer to that of experts. In effect, the video device acted as a built‑in guide, encouraging body and gaze habits associated with higher skill.
What this means for training and patient safety
For the layperson, the message is that expert skill is not just about quick hands, but also about how a clinician stands and where they look. This study shows that experienced doctors maintain a steady, slightly distant viewpoint during intubation, while beginners often hunch forward and narrow their focus. Video laryngoscopes appear to nudge novices toward the expert pattern, helping them keep their heads still and their field of view stable. By turning these subtle habits into measurable numbers, educators can design clearer teaching methods and potentially reduce errors during one of medicine’s most critical emergency procedures.
Citation: Yasuda, Y., Takehara, S. & Inoue, S. Quantitative analysis of gaze and body movement differences by proficiency in direct and video laryngoscope intubation. Sci Rep 16, 15656 (2026). https://doi.org/10.1038/s41598-026-44432-5
Keywords: tracheal intubation training, video laryngoscope, eye tracking, motion capture, medical education