Clear Sky Science · en
Adherence to Barrett’s esophagus surveillance guidelines and its impact on progression: a multicenter prospective study
Why this matters for everyday health
Barrett’s esophagus is a condition linked to cancer of the food pipe, so people who have it often face years of regular camera tests of the throat and stomach. This study asks a simple but important question: are those repeat tests being done as often as guidelines suggest, or more often than needed, and does extra testing actually help catch dangerous changes earlier?
What Barrett’s esophagus is
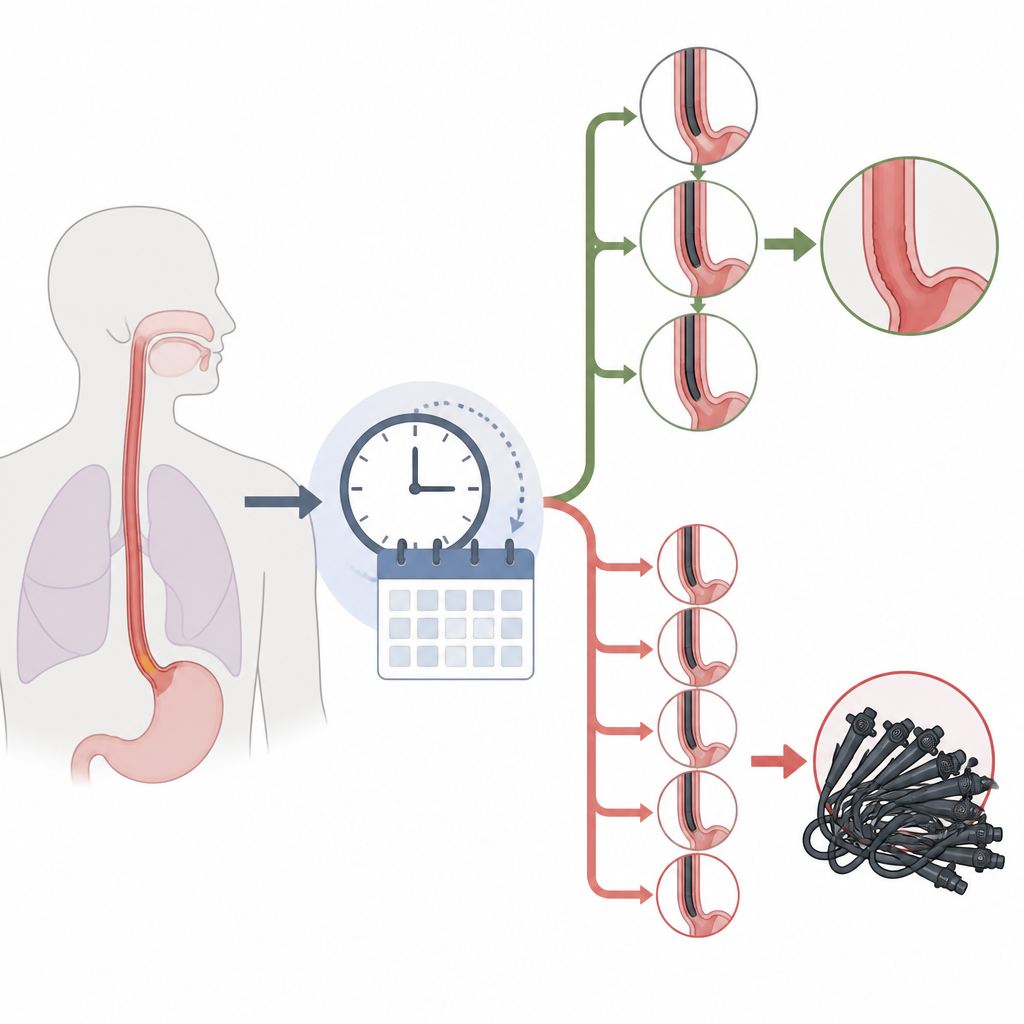
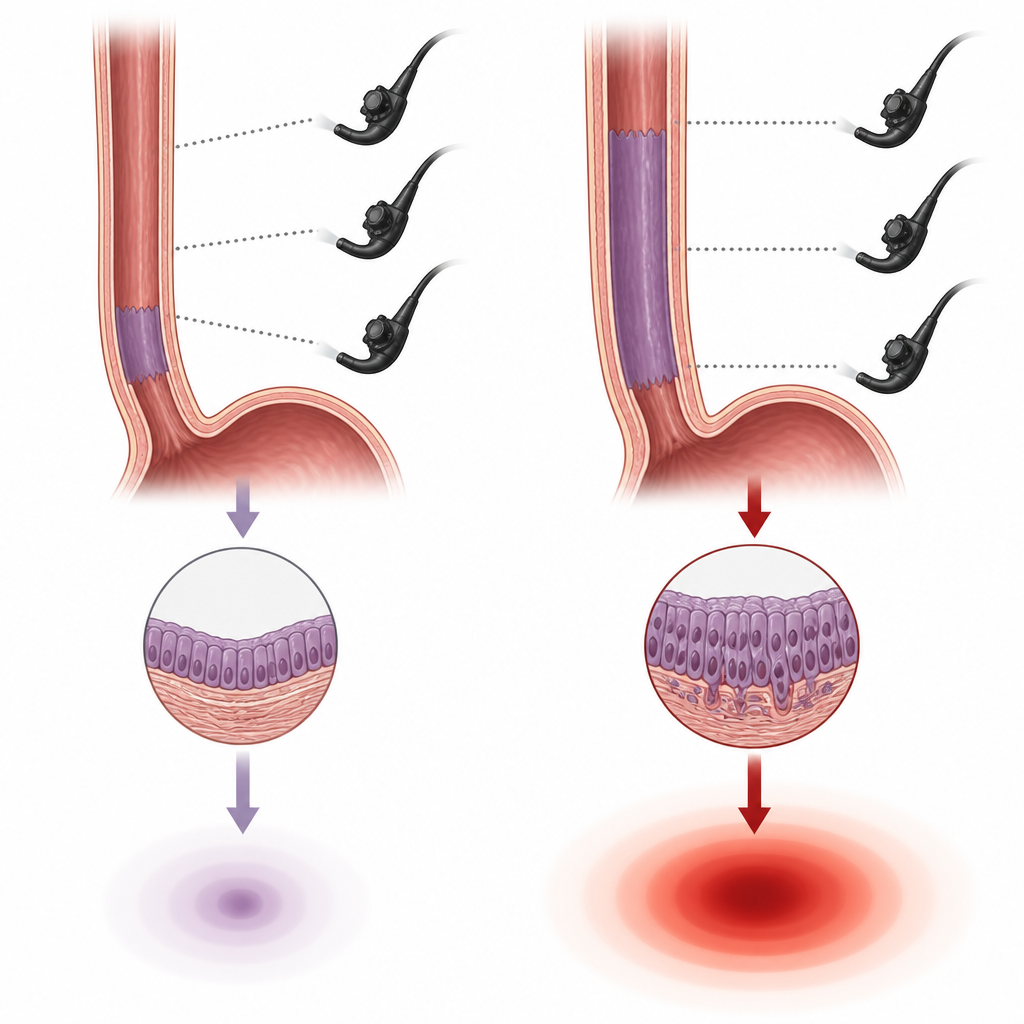
In Barrett’s esophagus, the normal lining of the lower food pipe is replaced by a different type of lining, often after years of acid reflux. This change slightly raises the chance of developing a serious cancer called esophageal adenocarcinoma. Because the cancer usually appears step by step, doctors recommend regular endoscopy checkups to spot early warning signs. Different expert groups have issued schedules for how often people should be checked, depending on how long the Barrett’s segment is and whether any abnormal cells have already been seen.
How the study was carried out
Researchers in Spain followed 375 adults with Barrett’s esophagus at 15 hospitals between 2016 and 2022. None had already been treated for Barrett’s or had early cancer at the start. Over a median of just over four years of follow up, these patients underwent 556 upper endoscopies, 505 of them done purely for routine surveillance. The team compared the actual timing of each surveillance test with what current guidelines advised, and they also tracked which patients’ Barrett’s tissue progressed to more abnormal or cancerous stages.
Too many early tests, few late ones
The study found that fewer than half of the surveillance endoscopies were done within the recommended time window. Just over 40 percent were on schedule, while about 50 percent were carried out earlier than guidelines suggested, and only 9 percent were delayed. When there was no solid medical reason for moving a test forward, the researchers labeled it “oversurveillance”; this applied to nearly one in three surveillance procedures. Shorter Barrett’s segments under 3 centimeters and referrals made by surgeons rather than gastroenterologists were linked to having tests done too early. In contrast, use of a careful biopsy method known as the Seattle protocol and other markers of high quality endoscopy were tied to better respect of the recommended timing.
Did extra endoscopies improve safety?
Over the follow up period, only 13 patients (about 3.5 percent) showed clear worsening of their Barrett’s tissue, with a yearly progression rate under 1 percent. Six of these developed advanced precancerous changes or cancer itself. The key factor linked to progression was how long the Barrett’s segment was: longer segments carried much higher risk, while age and follow up duration showed weaker links and smoking did not stand out. Crucially, patients who underwent early endoscopy did not have their dangerous changes detected more often than those who were scoped on time or a bit late. Even among people who were clearly oversurveilled, progression rates were similar.
What this means for patients and doctors
For people living with Barrett’s esophagus, these results suggest that more frequent camera tests do not automatically mean better protection. In this Spanish group, following guideline schedules would likely have avoided many procedures without missing important disease changes, especially in those with shorter Barrett’s segments whose overall risk was low. The study supports a more measured approach: focus careful, high quality surveillance on patients with longer segments and higher risk, while avoiding unnecessary repeat endoscopies that add cost, inconvenience, and small but real risks without clear benefit.
Citation: Murzi-Pulgar, M., Huerta, A., Sánchez-Montes, C. et al. Adherence to Barrett’s esophagus surveillance guidelines and its impact on progression: a multicenter prospective study. Sci Rep 16, 14945 (2026). https://doi.org/10.1038/s41598-026-44028-z
Keywords: Barrett’s esophagus, endoscopy, surveillance guidelines, esophageal cancer risk, Spain multicenter study