Clear Sky Science · en
Diagnostic efficacy of endoscopic ultrasound-guided fine needle aspiration cytology in pancreatic lesions
Why this matters for patients and families
Pancreatic problems can range from harmless cysts to aggressive cancers, yet they often cause similar vague symptoms like stomach pain, indigestion, or jaundice. Doctors need a safe, accurate way to tell which patients require urgent treatment and which can be watched or reassured. This study looks at a modern, minimally invasive test that uses an ultrasound camera inside the gut to guide a thin needle into the pancreas and sample suspicious spots, helping to answer that crucial question: “Is it cancer or not?” 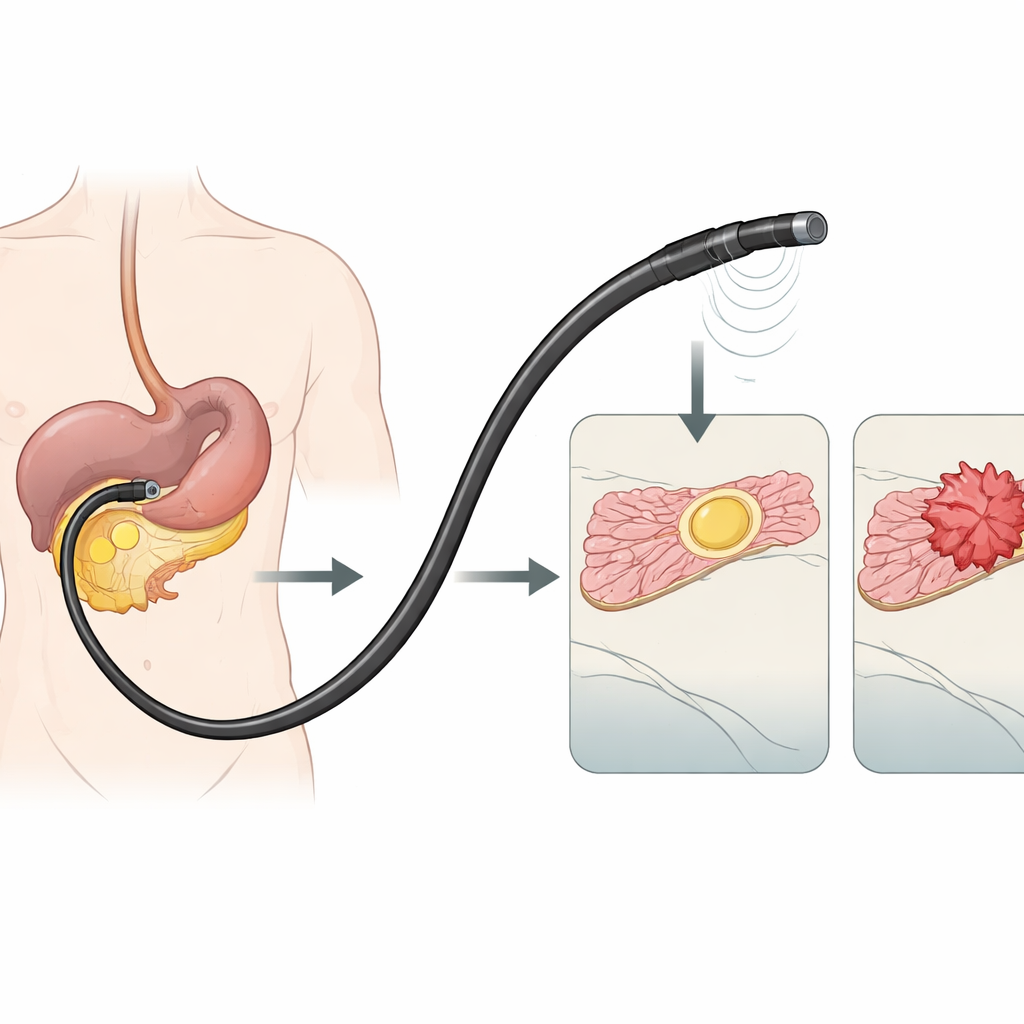
A closer look inside the body
The technique studied is called endoscopic ultrasound–guided fine needle aspiration, or EUS-FNA. Instead of making an incision, a flexible tube with a tiny ultrasound probe at its tip is passed through the mouth into the stomach and small intestine, which lie right next to the pancreas. Using live ultrasound pictures, the doctor threads a hair-thin needle through the wall of the gut directly into a suspicious lump in the pancreas. A small amount of tissue and cells is gently sucked into the needle. These samples are then examined under the microscope by specialists who look for signs of cancer or other diseases. In this study from a large hospital in eastern India, 67 people with lumps seen on scans of the pancreas underwent this combined camera-and-needle procedure.
How the study was done
All participants already had a pancreas lesion spotted on regular imaging such as ultrasound or CT. During a single session under sedation, doctors first performed EUS-FNA to collect loose cells for microscopic study, then immediately took a tiny core of tissue with a slightly larger needle. The loose-cell samples were reported using two different international systems: an older one from the Papanicolaou Society and a newer seven-level system from the World Health Organization (WHO). The tissue cores, examined separately, were treated as the “gold standard” final answer. By comparing the needle-cell results with the tissue results, the researchers could judge how often the test correctly identified cancer and how often it misled doctors.
What the test got right and wrong
Most of the lumps turned out to be located in the head and body of the pancreas, and patients were typically in their fifties and sixties, with more men than women affected. When the cell samples were classified using the older Papanicolaou system, the test picked up about 85 out of 100 cancers (its sensitivity) and correctly reassured about 60 out of 100 people who did not have cancer (its specificity). When the same slides were reinterpreted with the newer WHO system, both sensitivity and specificity improved to around the mid-80 percent range. The study also revealed why some readings were wrong. False alarms (benign growths called pseudocysts, solid pseudopapillary tumors, or reactive cell changes that mimicked cancer) often came from bloody or distorted samples that were hard to interpret. Missed cancers usually resulted from too few cancer cells being captured by the thin needle, even though the tissue biopsy taken at the same time showed the disease clearly. 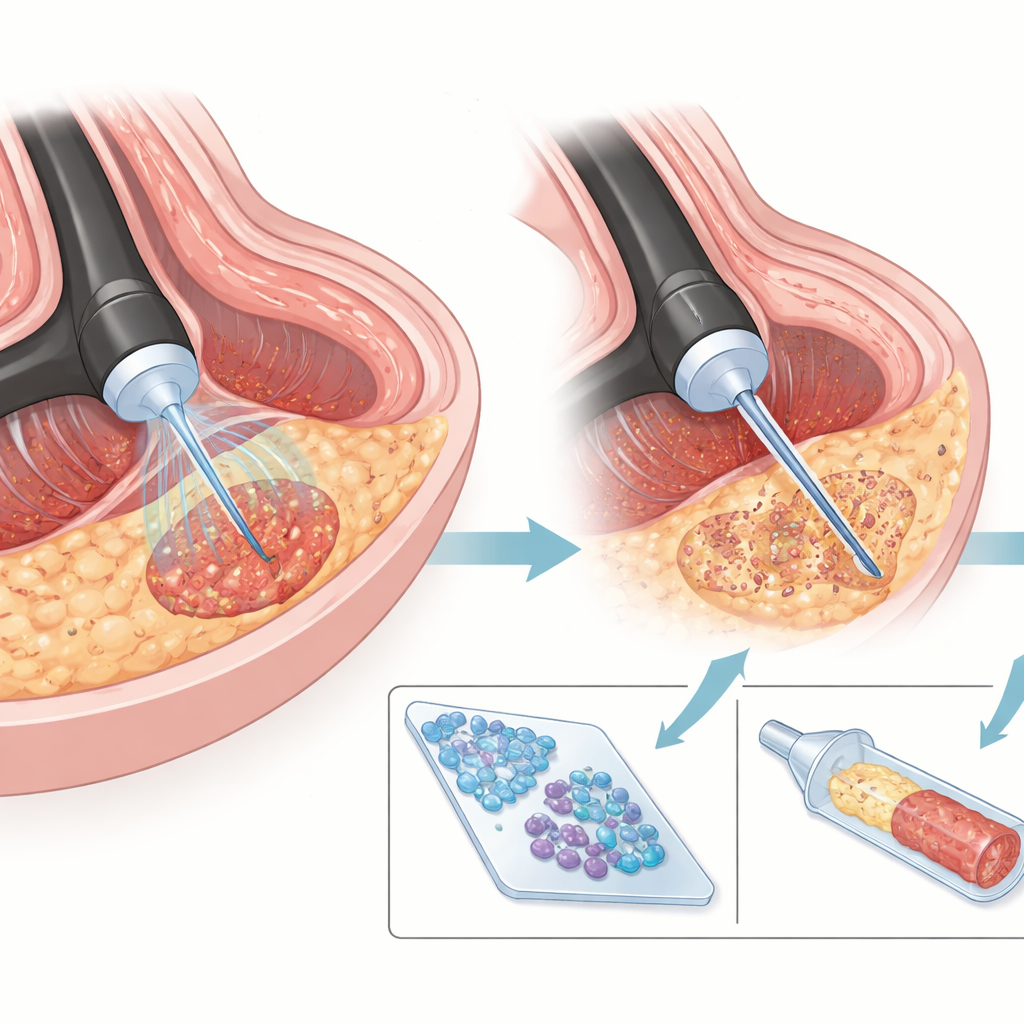
What this means for diagnosis and treatment
Because the pancreas sits deep in the abdomen and is surrounded by vital organs and blood vessels, traditional surgery or open biopsies carry real risks. This work reinforces that EUS-FNA offers a safer, more targeted alternative that can still provide crucial answers. It allows doctors to sample small or awkwardly placed lesions, distinguish long-standing inflammation from true tumors, and identify special tumor types such as hormone-producing growths that may benefit more from medicines than from major operations. Pairing the cell-based test with small tissue cores and additional staining techniques further sharpens the picture, especially for unusual cancers and rare pancreatic tumors.
Take-home message for non-specialists
For people facing the frightening possibility of pancreatic cancer, this study offers cautious reassurance. It shows that carefully performed, ultrasound-guided needle sampling from inside the gut can reliably separate many harmless or treatable pancreatic conditions from dangerous cancers, often in a single, short procedure. While it is not perfect and still depends on experienced operators and pathologists, the approach reduces the need for more invasive surgery just to get a diagnosis, and the newer WHO reporting system appears to make the test even more trustworthy. In practical terms, that means more patients can get an accurate answer sooner, and doctors can move quickly toward the right treatment plan or avoid unnecessary operations.
Citation: Mohanty, P., Dehuri, P. & Narayan, J. Diagnostic efficacy of endoscopic ultrasound-guided fine needle aspiration cytology in pancreatic lesions. Sci Rep 16, 13197 (2026). https://doi.org/10.1038/s41598-026-43859-0
Keywords: pancreatic lesions, endoscopic ultrasound, fine needle aspiration, cancer diagnosis, minimally invasive biopsy