Clear Sky Science · en
Biomechanical investigation of spinal cord stress changes following ACAF for different subtypes of cervical OPLL
Why Neck Nerve Pressure Matters
Neck pain, numb hands, or clumsy walking can sometimes trace back to a slow, silent process inside the spine: extra bone growing where a soft ligament should be. This condition, called cervical OPLL, can squeeze the spinal cord and the nerves that branch out to the arms. Surgeons now have a newer operation, ACAF, that slides this bony block forward instead of carving it away piece by piece. This study used advanced computer modeling to ask a practical question that affects real patients: how much space does the spinal cord actually need, and does the answer change with different shapes of bony overgrowth?
Different Ways Bone Can Crowd the Cord
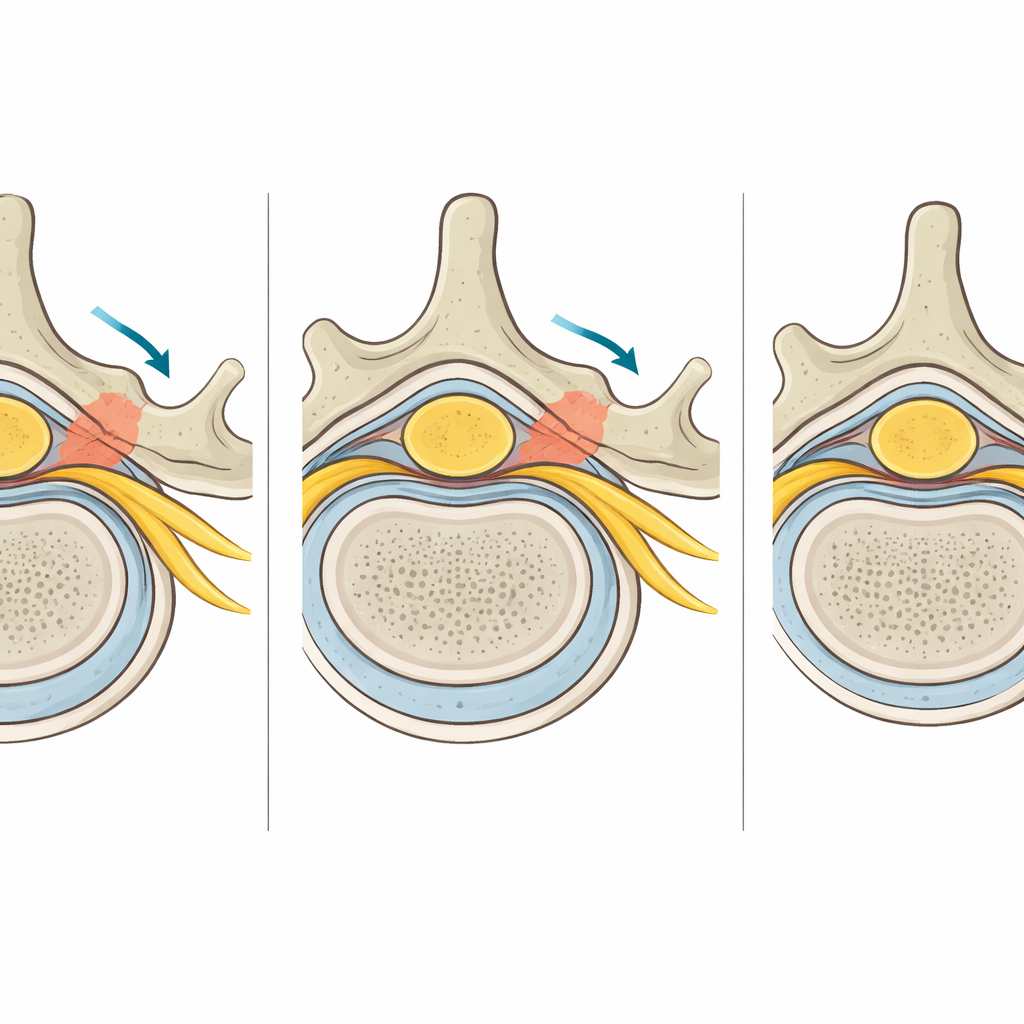
In cervical OPLL, a ligament that runs along the back of the vertebral bodies in the neck gradually turns to bone and bulges into the spinal canal. The authors focused on three common shapes of this overgrowth: a broad, flat “plateau” in the center; a pointed “beak” in the center; and a one-sided “beak” off to the right. Each shape crowds the cord and nearby tissues in a different way. Using detailed CT scans from a healthy volunteer, the team built a three-dimensional digital model of the C2–C7 vertebrae, spinal cord, its coverings, and the exiting nerve roots. They then “grew” these three OPLL shapes into the model and applied realistic material behaviors to the soft tissues, bone, and spinal fluid.
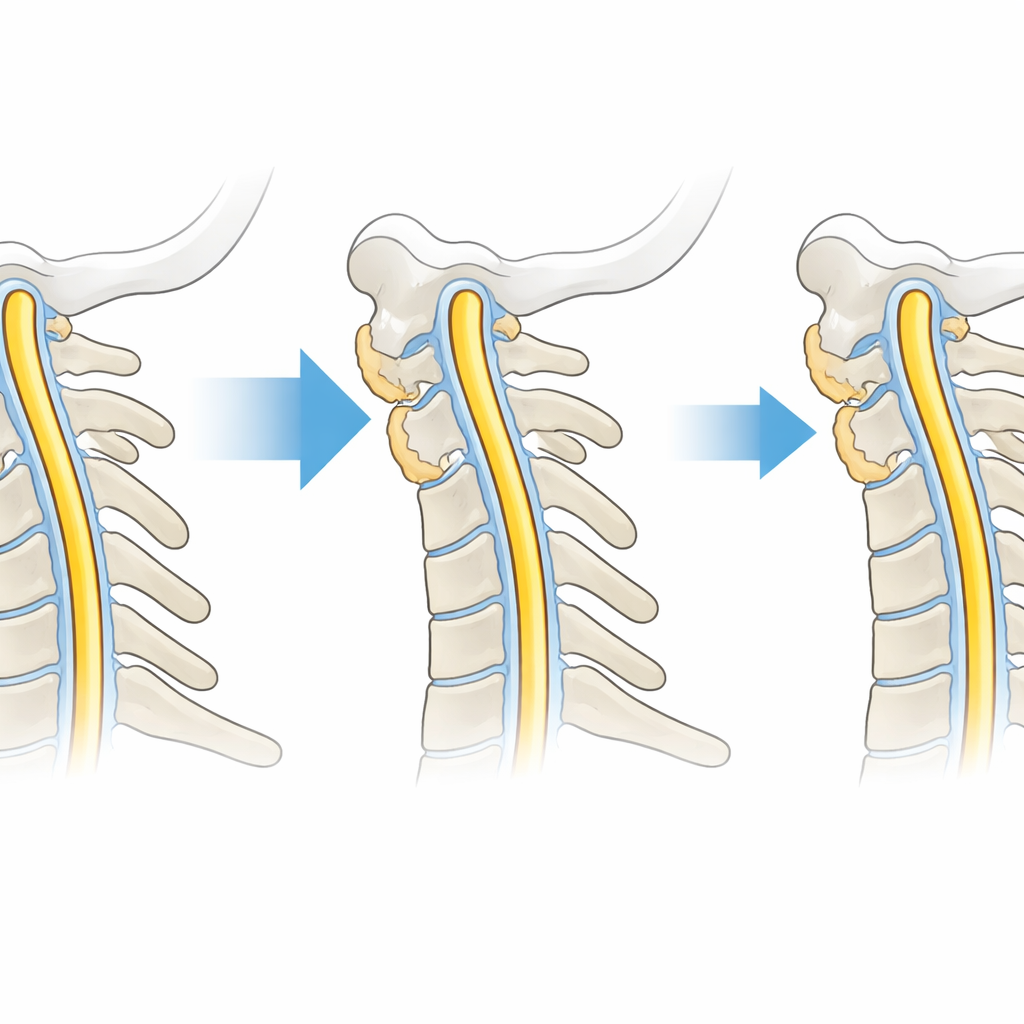
A Virtual Trial of a New Neck Operation
The operation under study, ACAF (Anterior Controllable Antedisplacement and Fusion), does not remove the bony overgrowth outright. Instead, surgeons partially shave the front of the vertebrae, free the block of vertebra plus ossified ligament, and pull this entire complex forward with a plate and screws. In the computer model, the researchers mimicked this by gradually shifting the ossified block toward the front of the neck. They measured how much mechanical stress was present in the gray and white matter of the spinal cord, the nerve roots, and the tough outer covering called the dura as the amount of canal “encroachment” by OPLL was reduced from a severe 60% down stepwise to 0%.
How Stress Eases as Space Opens Up
At the starting point, with 60% of the canal occupied, the central plateau type produced the highest stress inside the spinal cord itself, while the one-sided beak produced the greatest stress on the nerve roots and the dura on its own side. As the simulated ACAF procedure progressively moved the bony block forward, stress dropped in all tissues and in all three OPLL shapes. For the broad central plateau, stress in the gray and white matter fell sharply as encroachment dropped from 60% to about 30%, then declined much more slowly after that. For the one-sided beak, the largest gains were seen in nerve roots and dura as encroachment decreased from 60% to 40%, but some regions of the affected nerve root stayed under higher stress longer because of the angled, asymmetric pressure. Across types, the relief of pressure on the cord and its coverings began to look similar once the remaining encroachment became small.
A Potential Sweet Spot for Surgical Decompression
By tracking how mechanical stress changed with each step of decompression, the model suggested an important pattern: once the remaining bony encroachment was reduced to about 30% of the canal diameter, the extra benefit of pushing the block further forward became modest. Below this point, the stress in the spinal cord, nerve roots, and dura often plateaued rather than continuing to fall steeply. This does not mean 30% is a universal safety line for every patient, but it hints at a biomechanical “sweet spot” where most of the cord has been protected from harmful pressure.
What This Means for Patients and Surgeons
To a layperson, the message is that this newer ACAF surgery can meaningfully relieve pressure on the spinal cord and nerves for several common shapes of OPLL, and that most of the mechanical benefit may be gained once the bony overgrowth is reduced to roughly one-third of the canal or less. However, the authors stress that this number comes from a computer model, not from tracking real patients over time. Decisions about how aggressively to decompress still have to weigh symptoms, imaging, and surgical risks. Even so, this work offers surgeons a clearer, physics-based picture of how much breathing room the spinal cord gains with each incremental step of ACAF, and how that picture shifts with the exact shape and position of the offending bone.
Citation: Zhang, X., Gu, W., Cao, D. et al. Biomechanical investigation of spinal cord stress changes following ACAF for different subtypes of cervical OPLL. Sci Rep 16, 13740 (2026). https://doi.org/10.1038/s41598-026-43810-3
Keywords: cervical OPLL, spinal cord decompression, ACAF surgery, cervical myelopathy, finite element modeling