Clear Sky Science · en
Adaptable, quantitative CRISPR/Cas12a-based assay for cytomegalovirus DNA in infant saliva
Why a baby’s spit can tell an important story
For most newborns, a bit of drool is nothing to think about. But hidden in some infants’ saliva is cytomegalovirus (CMV), a common virus that can quietly damage hearing and brain development. Today, confirming CMV infection usually depends on polymerase chain reaction (PCR) machines that are expensive, slow, and often out of reach in places that need them most. This study describes a new laboratory method that uses CRISPR technology to measure CMV DNA in infant saliva more quickly and at lower cost, with an eye toward making early screening possible in both well-equipped hospitals and resource-limited clinics.

A silent infection with lifelong impact
CMV is a widespread virus that usually causes mild or no symptoms in healthy adults, but it can be devastating when passed from mother to baby during pregnancy. Congenital CMV infection is the leading non-genetic cause of childhood hearing loss worldwide and can also lead to problems with growth, vision, and development. Many infected babies look healthy at birth, and some do not show hearing loss until months or years later. Detecting the virus early, especially within the first three weeks of life, is critical because viral load—the amount of virus in the body—helps guide treatment decisions and may clarify whether an infection began before or after birth. Yet in many hospitals, especially in low- and middle-income countries, PCR testing is too costly or too slow to be used for universal newborn screening.
Turning gene-editing tools into virus detectors
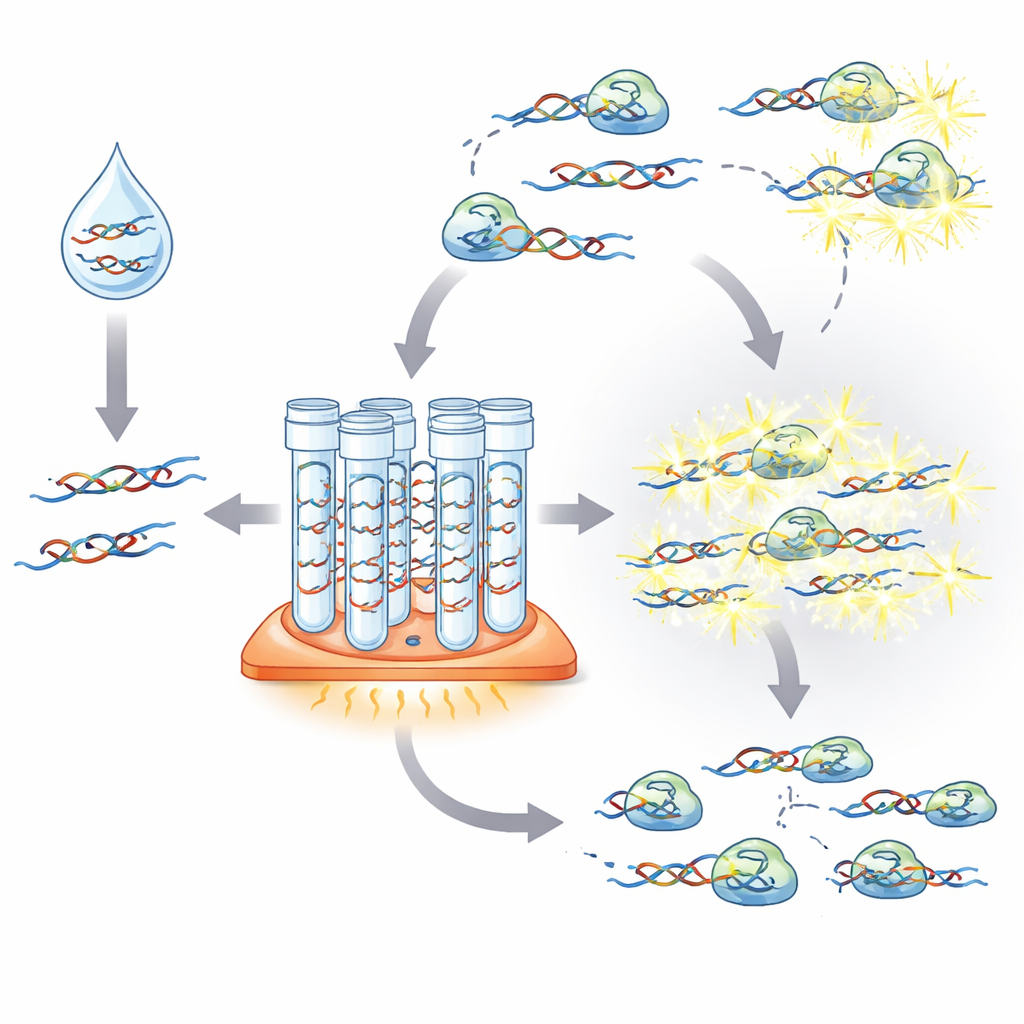
The researchers built a CMV test around two key pieces of technology that work at a single, gentle temperature, making them simpler than standard PCR. First, recombinase polymerase amplification (RPA) makes many copies of CMV DNA from a tiny starting amount. Second, CRISPR/Cas12a acts as a molecular sensor: once guided to the specific CMV gene segment, activated Cas12a begins cutting nearby “reporter” DNA fragments, generating a fluorescent signal that can be read by instruments. By adapting a well-established CMV PCR target region to this CRISPR-based format and carefully tuning reaction times and component concentrations, the team produced a two-step assay that can detect clinically meaningful levels of CMV in synthetic and plasma-based samples.
From precision instruments to portable readers
To see whether this approach could be practical outside advanced laboratories, the team tested several ways to read the fluorescent signal. A standard microplate reader in a university lab achieved detection limits similar to PCR, and simple mathematical models allowed viral loads to be estimated reasonably well in contrived samples. A smaller, lower-cost fluorometer preserved this ability to estimate viral load, but needed higher virus levels to register a clear signal. Lateral flow strips—similar in appearance to home pregnancy tests—could detect very low virus levels but only provided a yes-or-no answer, not a precise quantity. The scientists also explored a simplified sample-treatment method called HUDSON that avoids traditional DNA extraction, showing that CMV DNA can be detected directly in spiked saliva, though with reduced accuracy for precise quantification.
Putting the test to work in Sierra Leone
Because CMV burden is high in low-resource settings, the team partnered with Kenema Government Hospital in Sierra Leone to see how the assay would perform in a real-world clinical laboratory. Local technicians were trained to run the CRISPR-based protocol and use portable readers. Using synthetic CMV DNA, all technicians achieved similar results, demonstrating that the method is robust across different users and sites. The crucial test came with actual infant saliva samples collected in Sierra Leone. Here, the CRISPR assay’s estimates of viral load did not match PCR as closely as they had in controlled samples, likely because of biological differences in saliva and technical variability in the amplification step. Nonetheless, when used simply to classify samples as CMV-positive or CMV-negative, the assay reached about 87% sensitivity and 82% specificity compared with PCR—performance considered acceptable for a first-line screening tool.
A step toward broader newborn screening
The authors conclude that their CRISPR/RPA platform is not yet ready to replace PCR for precise CMV viral-load measurement in individual patients, but it already meets key benchmarks for a population-level screening test. They envision a “tiered” approach: an inexpensive, rapid CRISPR-based assay used on all newborn saliva samples, followed by confirmatory PCR only for those that test positive. This could drastically reduce costs, speed up identification of infected babies, and make large CMV studies feasible in places where PCR machines are scarce. With further optimization of the chemistry, sample handling, and safeguards against contamination, similar assays could help bring advanced molecular diagnostics to clinics around the world, turning a simple saliva sample into an early warning system for a lifelong health risk.
Citation: Chao, K., Dietrich, M.L., Covey, S.C. et al. Adaptable, quantitative CRISPR/Cas12a-based assay for cytomegalovirus DNA in infant saliva. Sci Rep 16, 13452 (2026). https://doi.org/10.1038/s41598-026-43462-3
Keywords: congenital cytomegalovirus, CRISPR diagnostics, newborn screening, low-resource laboratories, viral load testing