Clear Sky Science · en
Preliminary ultrastructural analysis suggests phenotype-specific myofiber alterations in idiopathic inflammatory myopathies
When Muscles Weaken Without a Clear Cause
Many people live with mysterious muscle weakness that can make it hard to climb stairs, lift objects, or even swallow. In a group of rare autoimmune conditions called idiopathic inflammatory myopathies, the body’s own defenses attack skeletal muscle, but doctors still struggle to match symptoms, lab tests, and biopsies into a clear picture. This study uses a powerful microscope technique to look at muscle fibers in unprecedented surface detail, hoping to reveal hidden patterns of damage that could one day improve diagnosis and treatment.
Looking at Muscle in a New Way
Traditionally, muscle samples from patients are examined with light microscopes, which show overall structure and inflammation but can miss fine details on the fiber surface. The researchers turned instead to scanning electron microscopy (SEM), which builds three-dimensional, high-resolution images of tissue. They analyzed 78 muscle biopsies taken from the thigh (quadriceps) and shoulder (deltoid) in patients with several forms of inflammatory muscle disease, including dermatomyositis, polymyositis, immune-mediated necrotizing myopathy, and inclusion body myositis, alongside a small control group. Their goal was to describe, in a systematic way, the tiny architectural changes in individual muscle fibers and to see whether distinct disease types showed distinct damage patterns.
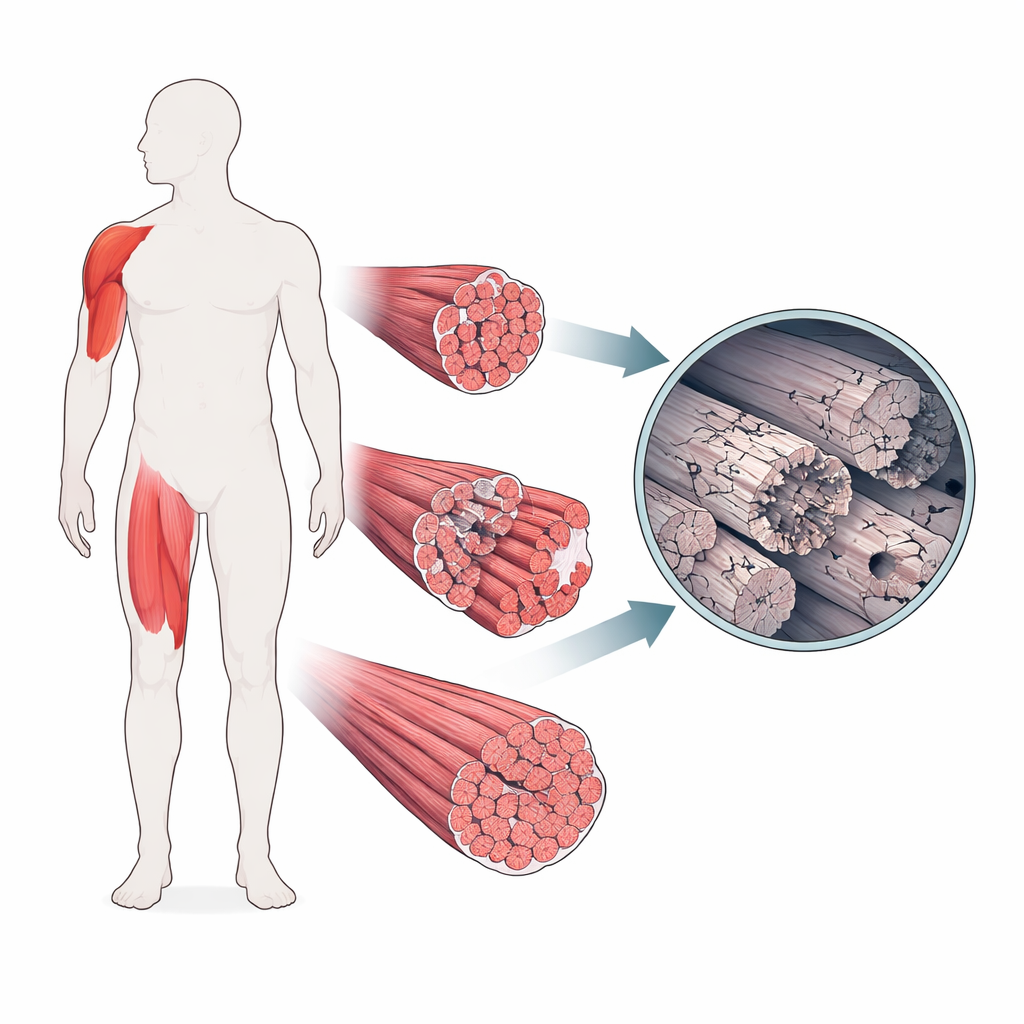
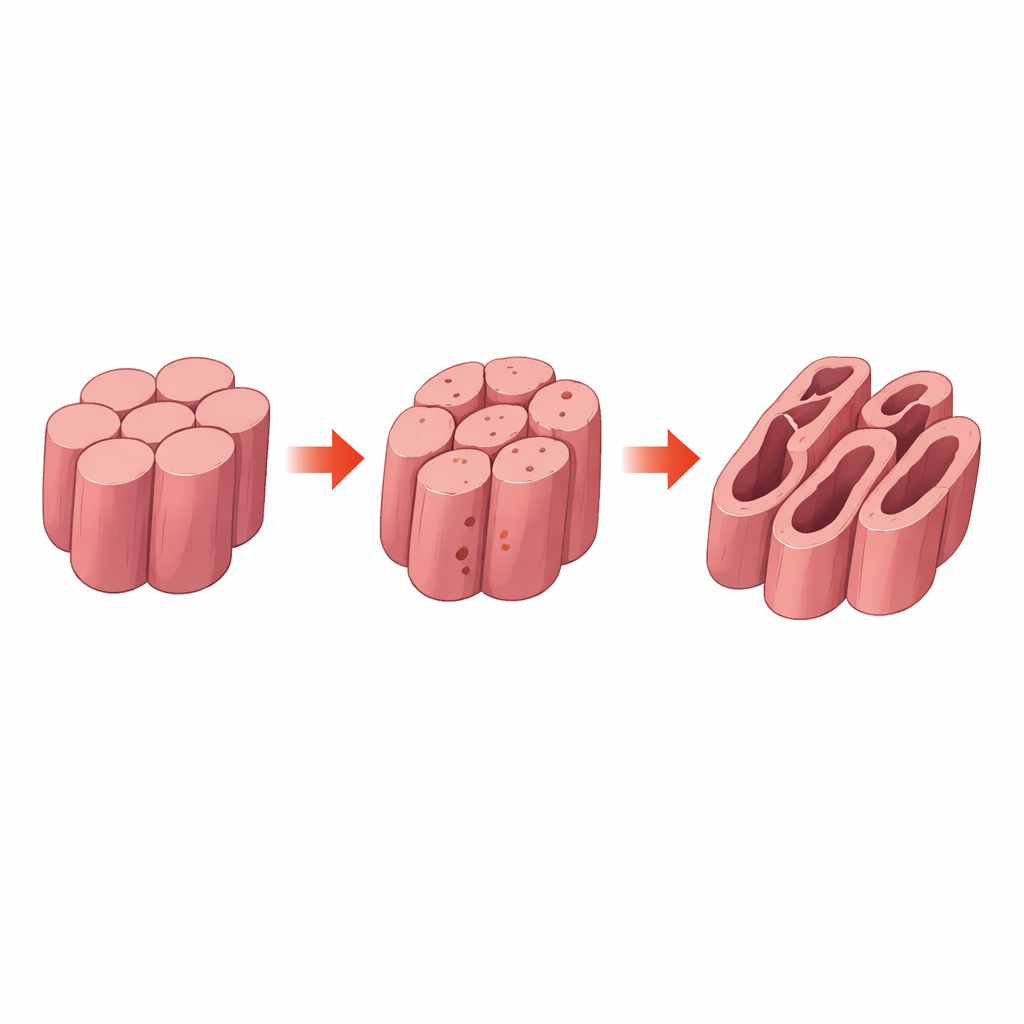
Tiny Holes, Cracks, and Tunnels in Muscle Fibers
Under SEM, the scientists defined several recurring features on muscle fibers: loss of the usual tightly packed, hexagon-like arrangement; differences in fiber size; small round pits on the surface (porosities); longer surface cracks (ruptures); deep tunnel-like defects running along fibers (perforations); and empty tubular spaces where whole fibers appeared to have disappeared (sarcolemma remnants). Loss of regular shape and variation in fiber size were seen in virtually all patients, but the more dramatic changes behaved differently across diseases. In dermatomyositis, fibers often looked relatively smooth and intact, appearing more like those from control samples. By contrast, immune-mediated necrotizing myopathy frequently showed perforations, while inclusion body myositis was notable for sarcolemma remnants, suggesting fibers that had been hollowed out or lost altogether.
Linking Microscopic Damage to Symptoms and Blood Tests
The team then asked whether these ultrastructural scars corresponded to how ill people actually were. In both quadriceps and deltoid muscles, porosities and ruptures tended to appear in patients with weaker muscles and higher levels of blood enzymes that leak out when muscle cells are injured, such as creatine phosphokinase and liver-associated enzymes. Interestingly, perforations were mostly found in samples that also showed necrosis—the outright death of muscle fibers—in standard stained sections, implying that these tunnels could be a surface sign of acute, destructive injury. In contrast, areas where muscle had long since been replaced by fat, a hallmark of chronic damage, showed fewer of these surface lesions, perhaps because there were fewer living fibers left to injure.
Different Muscles, Different Stories
The study also revealed that not all muscles are affected in the same way. Quadriceps samples more often showed porosities and ruptures and had greater variability in fiber size than deltoid samples, hinting that large weight-bearing muscles may be particularly vulnerable to structural disruption. When the researchers measured the cross-sectional area of individual fibers and compared them to published normal values, most patients—regardless of disease type—showed signs of fiber atrophy, meaning that fibers were, on average, smaller than in healthy muscle. Yet within this overall shrinkage, dermatomyositis again stood out: over time, these patients tended to have more normal-sized fibers and lower muscle enzyme levels, suggesting some degree of recovery or stabilization, in contrast to the more relentlessly damaging course seen in other myopathies.
What These Findings Mean for Patients
To a non-specialist, the takeaway is that muscle fibers in inflammatory myopathies do not all break down in the same way. Using SEM, the researchers uncovered distinct surface patterns—pits, cracks, tunnels, and empty tubes—that seem to align with particular disease subtypes and with how active the damage is. Dermatomyositis, despite its classic appearance under standard microscopy, may actually preserve much of its deeper muscle architecture, whereas other forms show more aggressive destruction. Although this work is preliminary and based on a modest number of patients, it suggests that high-resolution imaging of muscle could eventually help doctors distinguish between related diseases, gauge how active the damage is, and perhaps monitor responses to therapy more precisely than current tools allow.
Citation: Aguilar-Vazquez, A., Juarez-Gomez, C., Gonzalez-Gauna, E. et al. Preliminary ultrastructural analysis suggests phenotype-specific myofiber alterations in idiopathic inflammatory myopathies. Sci Rep 16, 12332 (2026). https://doi.org/10.1038/s41598-026-42717-3
Keywords: idiopathic inflammatory myopathies, skeletal muscle ultrastructure, scanning electron microscopy, dermatomyositis, muscle fiber damage