Clear Sky Science · en
Validation of the inferior vena cava collapsibility as a predictive marker of fluid responsiveness in spontaneously breathing patients
Why this matters for patients in intensive care
When someone is critically ill, doctors often give fluids through a drip to boost blood flow and support vital organs. Yet not every patient benefits from extra fluid, and too much can damage the lungs and other organs. This study explores a simple ultrasound check of a large vein in the abdomen as a way to judge in advance who is likely to respond well to a fluid boost, helping doctors choose treatment more safely.
Checking a major vein with bedside ultrasound
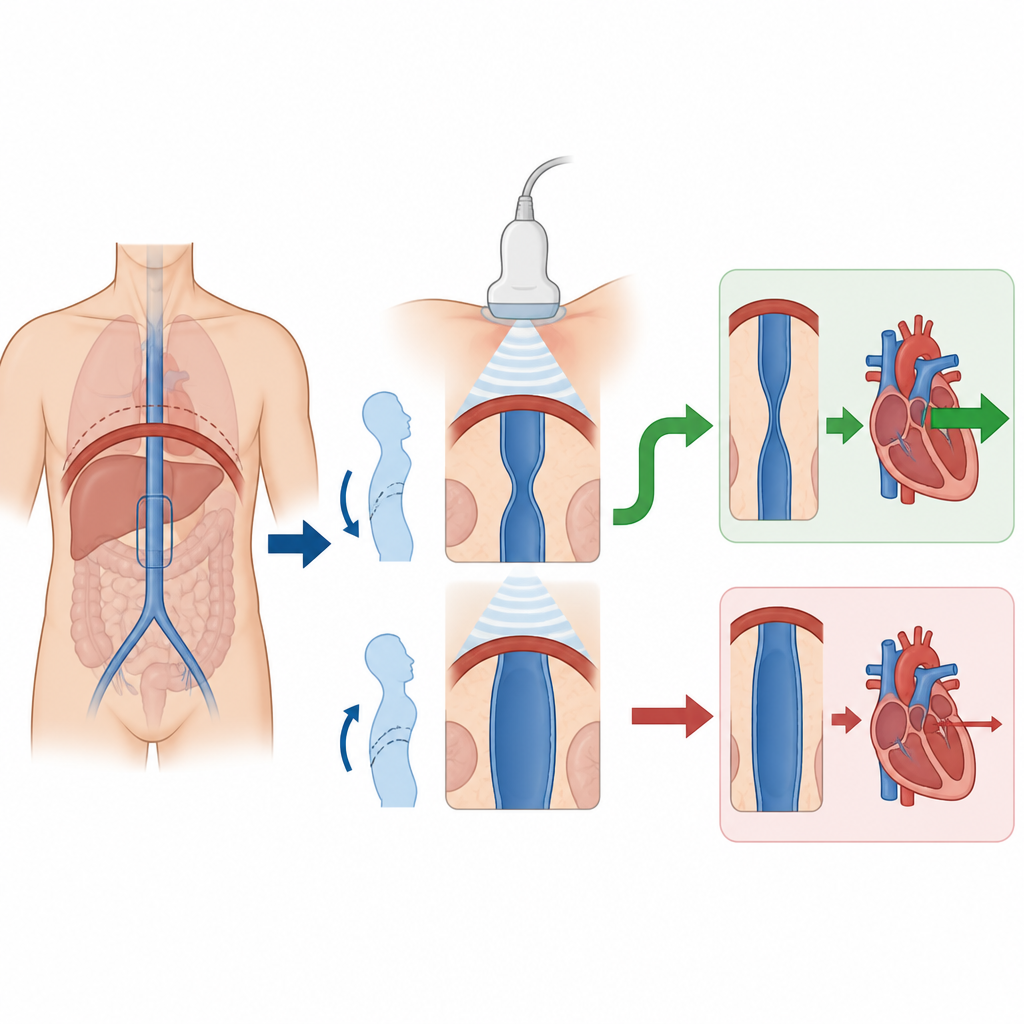
The research focuses on the inferior vena cava, a large vein that carries blood from the lower body to the heart. Its size changes with breathing. When a person breathes in, the vein can briefly narrow if the body is short on blood volume. Using a small ultrasound probe placed just below the breastbone, clinicians can watch this vein over several breaths and calculate how much it narrows. A high amount of narrowing suggests that the heart will pump more strongly if the patient receives extra fluid, while little change may mean further fluid will not help.
Testing normal and deep breaths
The investigators studied adults in intensive care units who were breathing on their own, not on a ventilator. They measured how much the vein narrowed during normal relaxed breathing and during a short, deeper breath that patients were asked to perform. At the same time, they used a known bedside test called passive leg raising, which briefly shifts blood from the legs toward the heart, to see whether the patient’s heart output increased. If blood flow rose by at least ten percent during leg raising, the patient was considered fluid responsive, meaning they would likely benefit from a real fluid infusion.
How well the vein test predicted benefit from fluids
Among 61 patients, 38 turned out to be fluid responsive by the leg raising test. The team then compared this to the ultrasound measurements. They had previously proposed two simple cutoffs: one based on normal breathing and one based on the deeper, more standardised breath. In this new group, the same cutoffs performed well. When the vein narrowed by at least about one third during normal breathing, the test correctly identified most patients who would respond to fluid and most who would not. During the deeper, standardised breath, an even larger amount of narrowing gave slightly better accuracy, with only a small number of patients misclassified.
Making the test practical at the bedside
The authors also examined how easy the approach was to use in real intensive care settings. Most patients were not on strong blood pressure drugs and were stable enough to cooperate with breathing instructions, similar to many people seen in emergency rooms or high-dependency wards. The ultrasound images could not be obtained in only a small minority, and measurements taken by different observers were highly consistent when a clear method was followed, including where exactly along the vein to measure. The researchers suggest a simple stepwise bedside rule: start with the vein measurement during normal breathing, and ask for the deeper breath only if the first result is not clearly above the higher cutoff.
What this means for everyday care
For people in intensive care who are breathing on their own, this study supports the idea that watching how a key abdominal vein narrows with breathing can help predict whether extra fluid is likely to improve blood flow. The method is non invasive, relies on widely available ultrasound equipment, and could reduce both under treatment and fluid overload. The authors conclude that while the simple test appears reliable, more work is needed to confirm exactly how much the added deep breathing step improves decision making in different groups of patients.
Citation: Ter Schiphorst, B., Bourel, C., Durand, A. et al. Validation of the inferior vena cava collapsibility as a predictive marker of fluid responsiveness in spontaneously breathing patients. Sci Rep 16, 15678 (2026). https://doi.org/10.1038/s41598-026-41826-3
Keywords: fluid responsiveness, inferior vena cava, critical care ultrasound, intensive care, passive leg raising