Clear Sky Science · en
A modified Yoong ultrasound guided injection for hydrodilation of subacromial subdeltoid bursa at the rotator interval for frozen phase of adhesive capsulitis
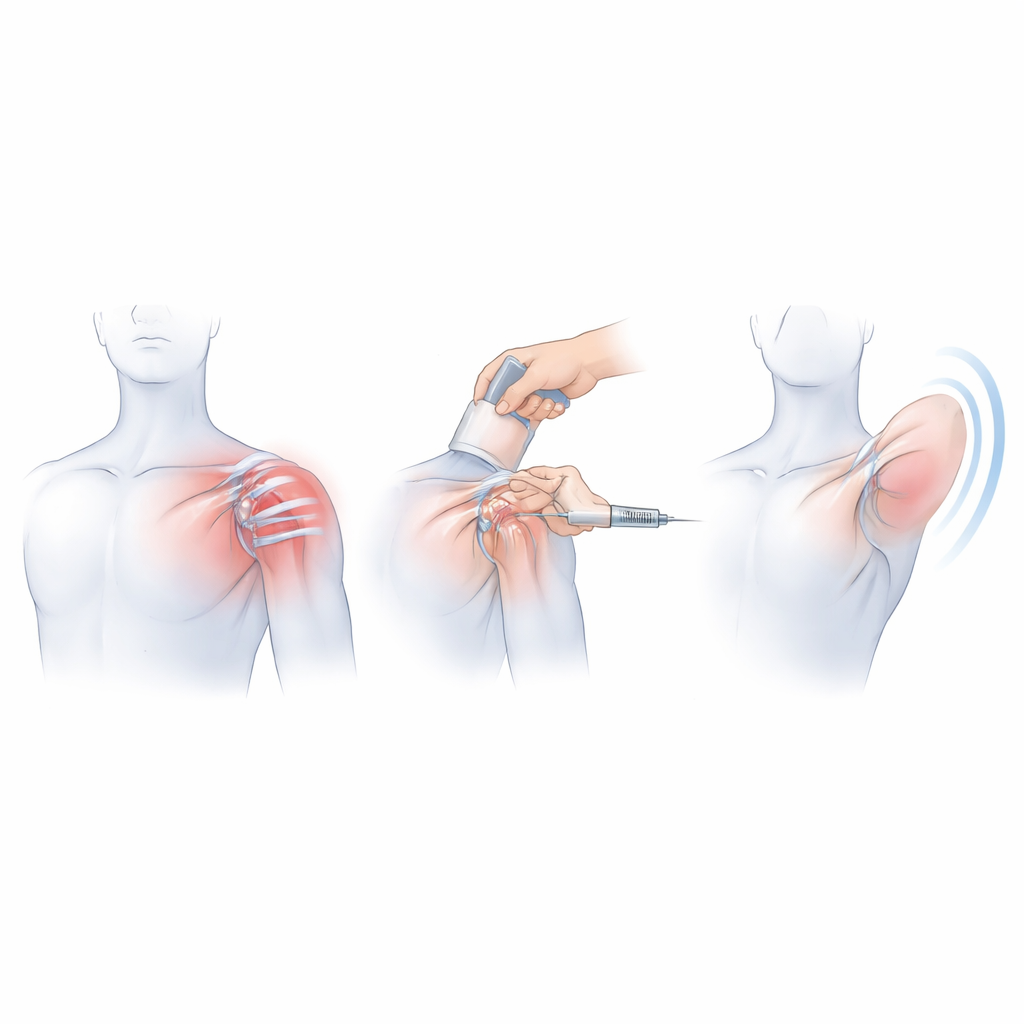
Why a stiff shoulder matters
Many people in midlife suddenly find that one shoulder becomes painfully stiff for months, sometimes years. This "frozen shoulder," or adhesive capsulitis, can make it hard to comb hair, reach overhead, or even get dressed. Doctors often use guided injections to ease pain and restore movement, but some of the current techniques can be difficult to perform and quite uncomfortable. This study describes a refined way to give an ultrasound‑guided injection that aims to be easier for clinicians, less painful for patients, and still highly effective in improving shoulder motion.
What happens in a frozen shoulder
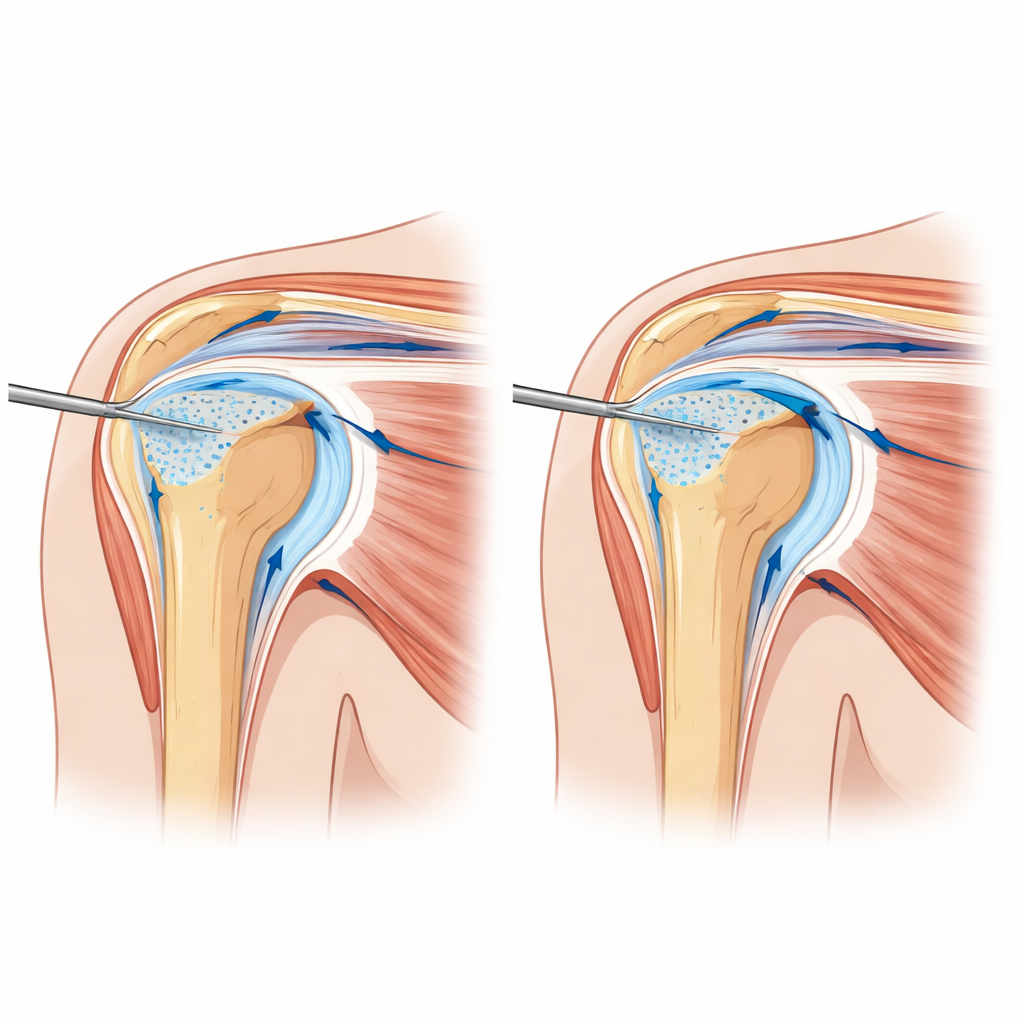
In frozen shoulder, tissue at the front of the joint becomes thick, tight, and inflamed. A key area is a small triangular zone called the rotator interval, which lies between two important shoulder tendons and houses several ligaments, the biceps tendon, and the front part of the joint lining. Imaging and surgical studies show that, in this region, one ligament in particular becomes thick and contracted, and the nearby sliding sac above the shoulder—the subacromial subdeltoid bursa—can turn fibrotic and swollen. Because this bursa is rich in pain‑sensing nerve endings, the authors argue that it may be a major source of pain and stiffness, especially in the so‑called frozen phase when movement is most restricted.
Why the usual injection can be a problem
Over the past decade, a popular treatment has been ultrasound‑guided “hydrodilatation” using a front‑of‑shoulder approach described by Yoong and colleagues. In that method, a needle is guided under the thickened ligament and into the joint space, where a mixture of fluid and steroid is injected under pressure to stretch the capsule. However, when the ligament is very thick and tight—as it often is in the frozen phase—pushing the needle and fluid through it can meet strong resistance and cause marked discomfort. There is also a real risk, especially for less experienced operators, of accidentally injecting into the nearby biceps tendon. Swelling of neighboring tendons can further narrow the target area, making the procedure technically demanding and time‑consuming.
A gentler path into the shoulder
To address these drawbacks, the authors propose a modified route that targets the subacromial subdeltoid bursa at the level of the rotator interval rather than the joint cavity itself. Under ultrasound, the patient lies on their back with the shoulder gently extended and rotated outward to open up the front of the joint. The operator first numbs the skin and bursal region, then advances a fine needle from the side toward the rotator interval while watching the tip in real time. After local anesthetic is given, the needle is used to gently perforate the thickened ligament multiple times—called fenestration—before being positioned just above it in the bursal space. A larger volume of mixed fluid (local anesthetic, dextrose solution, and corticosteroid) is then injected, spreading freely in the bursa and through the tiny perforations to bathe and soften the tight tissues. Because the needle does not have to force its way through a solid ligament into the joint, the injection tends to be smoother and less painful.
What the early results show
The team tested this technique in thirteen patients with frozen‑phase adhesive capsulitis seen over nine months in a sports medicine clinic. Most were women in their early fifties, and over half had diabetes, a common risk factor for frozen shoulder. After the injection, patients immediately performed simple guided movements and later began formal physiotherapy. Across follow‑up visits up to 24 weeks, their shoulder range of motion improved dramatically: average forward elevation roughly doubled, abduction increased from barely shoulder‑height to nearly full overhead, and outward rotation steadily improved. Pain scores dropped from moderate‑to‑severe at baseline to almost no pain by six months. No complications were reported, and the authors found the procedure quick to perform with a relatively shallow learning curve.
What this could mean for patients
For people struggling with a frozen shoulder, this modified injection offers a promising combination of comfort and effectiveness. By focusing on the pain‑sensitive bursa and stiff ligament at the rotator interval rather than forcing fluid directly into the joint, the method appears to reduce procedural discomfort while still unlocking motion and easing pain. The authors caution that their study is small and lacks a direct comparison group, so larger head‑to‑head trials are needed before the technique can be declared superior to existing methods. Still, these early results suggest that a more targeted, tissue‑softening approach to hydrodilatation may help many patients regain the simple, daily freedom of raising an arm without pain.
Citation: Mohamad, A.A., Mohamad, N. & Md Yusoff, B.A.H. A modified Yoong ultrasound guided injection for hydrodilation of subacromial subdeltoid bursa at the rotator interval for frozen phase of adhesive capsulitis. Sci Rep 16, 8881 (2026). https://doi.org/10.1038/s41598-026-41184-0
Keywords: frozen shoulder, adhesive capsulitis, ultrasound-guided injection, hydrodilatation, subacromial bursa