Clear Sky Science · en
Differentiating ischemic from healthy myocardium using cardiovascular magnetic resonance dipyridamole rest and stress T1 mapping
Seeing Heart Trouble Without Dyes
When doctors suspect clogged heart arteries, they often rely on magnetic resonance imaging (MRI) together with injected contrast dyes to see which parts of the heart muscle are starved of blood or scarred. But those dyes are not ideal for everyone, especially people with kidney problems or allergies, and they add time, cost, and environmental impact. This study explores a way to read the heart’s condition directly from the MRI signal itself, using a routine stress medicine called dipyridamole, so that damaged, threatened, and healthy heart muscle can be told apart without any contrast dye at all.
A New Way to Color the Beating Heart
Modern cardiac MRI can measure a property called T1, which behaves a bit like a built‑in color scale for heart tissue: water‑rich or injured areas show different T1 values than firm, healthy muscle. By taking T1 measurements at rest and during drug‑induced stress, doctors can watch how heart muscle responds when blood flow is pushed to its limits. Earlier work showed that stress tests using other medicines, such as adenosine or regadenoson, can reveal which regions are normal, temporarily deprived of blood (ischemic), or permanently scarred (infarcted). However, these drugs are not available or ideal everywhere. Dipyridamole, a long‑standing stress agent used in nuclear heart scans, is cheaper, widely used, and has a longer‑lasting effect, but its behavior in T1‑based MRI had not been fully tested.
Who Was Studied and How
The researchers examined 25 healthy volunteers and 20 patients with long‑standing coronary artery disease, all of whom underwent heart MRI in a 1.5‑Tesla scanner. Everyone first had T1 mapping at rest, then received an infusion of dipyridamole to widen their coronary arteries, followed by repeat T1 mapping under stress. In the patient group, the team also obtained conventional contrast‑enhanced scans and quantitative blood‑flow maps, allowing them to mark out regions of clearly scarred muscle, regions that became dark only during stress (indicating reversible ischemia), and “remote” regions that looked unaffected on standard images. For each type of tissue, they calculated both the T1 value at rest and the percentage change between rest and stress, a measure of how strongly the tissue responded.
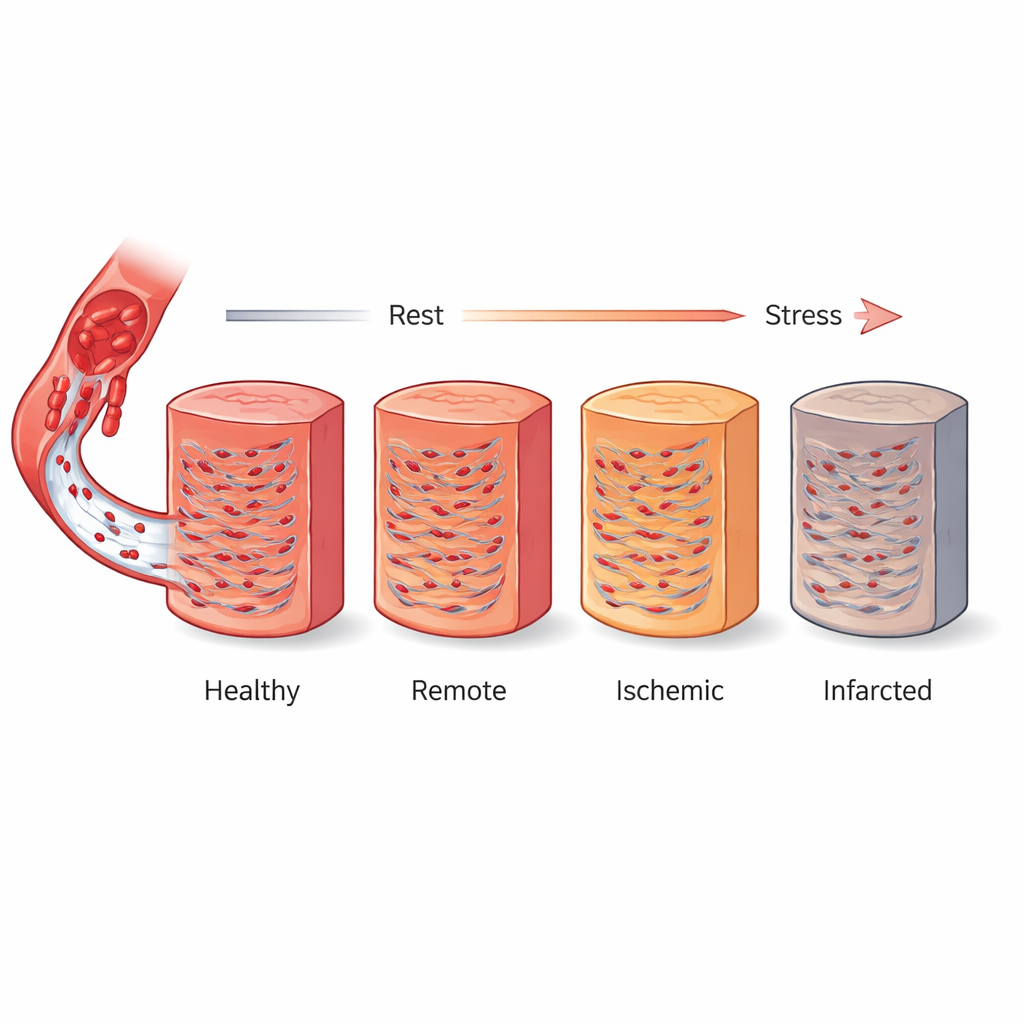
What the Heart’s Signal Revealed
In healthy volunteers, heart muscle showed a consistent rise in T1 with dipyridamole stress—about 6.5 percent on average—across all levels of the heart and across all major coronary territories. This rise likely reflects extra blood volume filling tiny vessels when the arteries are fully opened. In patients with coronary disease, the picture was more varied. Areas of old scar had clearly higher T1 values at rest and showed virtually no increase, or even a slight decrease, under stress, consistent with dead tissue that cannot recruit more blood. Ischemic regions had only mildly raised resting T1 but a very blunted stress response, while remote regions looked normal at rest yet still reacted less strongly than truly healthy muscle. Overall, the biggest T1 jump was seen in normal tissue, followed by remote, then ischemic, with almost no change in scar.
Linking MRI Signals to Blood Flow
Because the patient group also underwent full contrast‑based perfusion imaging, the team could compare their non‑contrast T1 results with direct measurements of blood flow. They found that the size of the T1 increase during stress tracked closely with both peak stress flow and the ratio of stress to rest flow, a common index of how well the coronary system can adapt to demand. There was no meaningful link between T1 change and resting flow alone. This pattern supports the idea that stress‑induced T1 changes mainly mirror how much extra blood volume can be recruited into the muscle’s microscopic vessels when the heart is challenged—precisely the reserve that is lost in diseased or scarred regions.
What This Could Mean for Patients
For people at risk of coronary artery disease, these findings suggest that a stress MRI using dipyridamole and T1 mapping could someday offer a dye‑free way to tell healthy, threatened, and dead heart muscle apart in a single, quantitative scan. While more work in larger, age‑matched groups is needed to set firm cut‑off values and refine automated analysis, this study shows that dipyridamole‑based stress T1 mapping can separate infarcted, ischemic, and normal myocardium and mirrors key blood‑flow measures. In the future, that could make cardiac MRI safer and more accessible for vulnerable patients, while reducing reliance on contrast dyes and still giving doctors a clear picture of how well the heart muscle is truly being supplied.
Citation: Chang, YT., Chien, CY., Huang, WM. et al. Differentiating ischemic from healthy myocardium using cardiovascular magnetic resonance dipyridamole rest and stress T1 mapping. Sci Rep 16, 8926 (2026). https://doi.org/10.1038/s41598-026-40946-0
Keywords: cardiac MRI, stress testing, coronary artery disease, myocardial ischemia, noncontrast imaging