Clear Sky Science · en
Identifying intact and fibrotic parenchyma in pancreatic ductal adenocarcinomas using compression optical coherence elastography
Why this matters for people facing pancreatic surgery
Pancreatic surgery is among the most demanding operations in medicine, and its success depends heavily on the condition of the remaining pancreas. If the tissue is too "soft," patients are more likely to develop a dangerous leak of digestive juices called a pancreatic fistula. At the same time, surgeons must be sure they have removed all of a pancreatic tumor without cutting away more healthy organ than necessary. This study presents a new imaging approach that lets doctors measure how stiff different parts of the pancreas are during surgery, potentially making these high‑stakes decisions safer and more precise.
Seeing how firm the pancreas really is
Today, surgeons usually judge pancreatic firmness by touch, pressing the organ gently with their fingers and deciding whether it feels "soft" or "hard." That impression influences how much tissue they remove and how they reconstruct the digestive tract. But touch is subjective, and the pancreas can be patchy, with normal, scarred, and cancerous areas side by side. The researchers explored a light‑based technique called compression optical coherence elastography, or C‑OCE, which can create a microscopic map of tissue stiffness in real time. By shining harmless infrared light into a small piece of freshly removed pancreas and gently compressing it, the system tracks how much different regions deform, translating this into a color‑coded stiffness image. 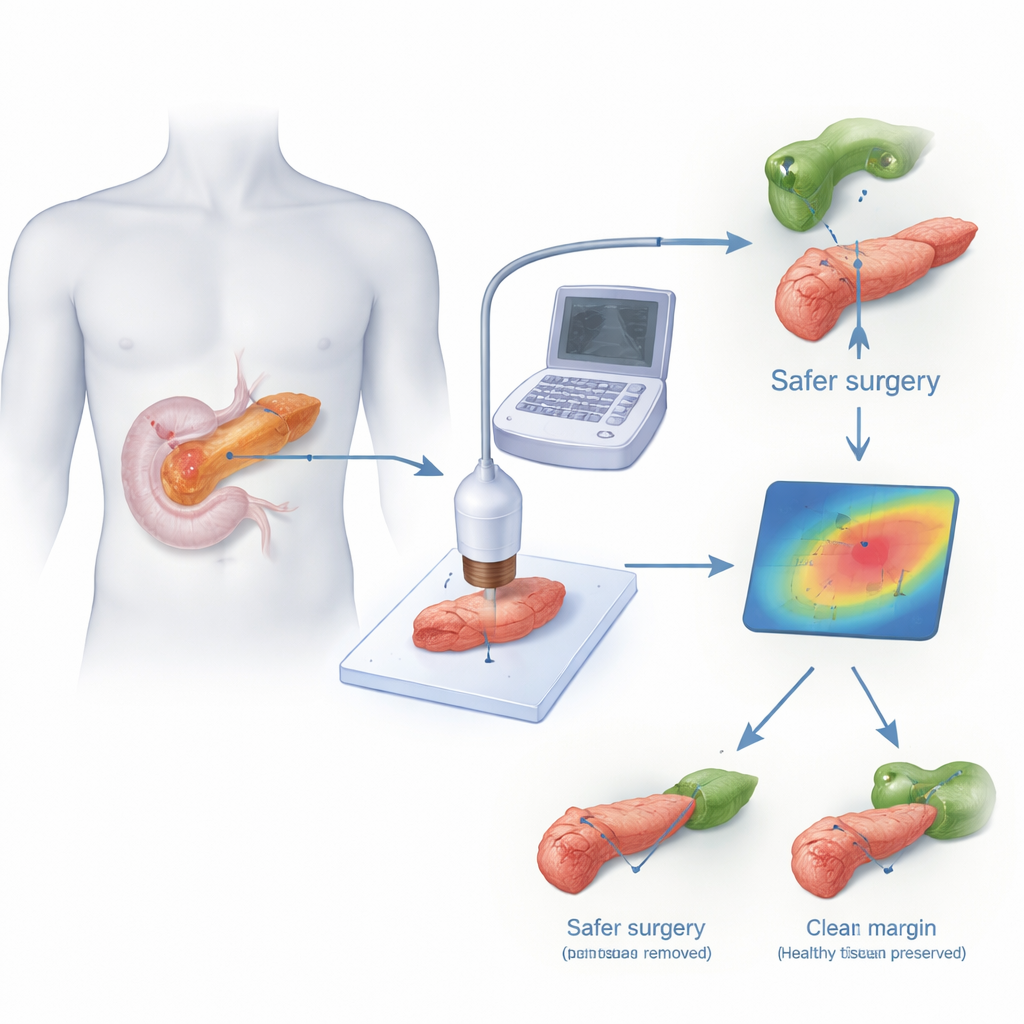
Measuring healthy, scarred, and cancerous tissue
The team studied 35 samples of human pancreas taken during surgery for pancreatic ductal adenocarcinoma, the most common form of pancreatic cancer. Each specimen contained tumor and nearby non‑tumor tissue. For every region imaged with C‑OCE, they later examined matching slices under the microscope to know exactly what kinds of tissue were present. They showed that the method could clearly distinguish fatty tissue, normal enzyme‑producing cells, fibrous scar tissue from chronic inflammation, the tiny hormone‑producing islets that regulate blood sugar, and the cancer itself, based on how stiff each was. Normal pancreatic tissue was relatively soft, fibrotic areas were substantially firmer, and tumors were the stiffest of all, with values several times higher than healthy regions.
Linking stiffness to surgical risks and islet transplant potential
One critical finding was the tight relationship between softness of the pancreas and the risk of postoperative pancreatic fistula. Patients whose pancreatic tissue measured below a certain stiffness threshold on C‑OCE were far more likely to develop this complication. Using a cutoff of 84 kilopascals, the test correctly identified most patients who did and did not go on to form a fistula, with high sensitivity and specificity. In contrast, the surgeon’s fingertip impression of "soft" versus "hard" often disagreed with the microscopic findings and with the C‑OCE measurements. The method also highlighted stiff little islands within softer tissue that corresponded to islets of Langerhans, the endocrine clusters that can sometimes be isolated and transplanted to help prevent diabetes after total removal of the pancreas. Being able to estimate how many viable islets are present, based on stiffness maps, could help decide when islet autotransplantation is worthwhile.
Finding the true edge of the tumor
Another major challenge in pancreatic cancer surgery is defining a clean boundary between tumor and non‑tumor tissue—the resection margin. Standard frozen‑section pathology samples only tiny areas and can miss cancer cells, especially after chemotherapy has altered the tissue. In this study, C‑OCE produced sharp transitions in stiffness at the interface between tumor and surrounding pancreas, both in untreated patients and in those who had received chemotherapy. Cancer regions showed very high stiffness, while nearby non‑tumor or treatment‑scarred tissue was clearly less rigid. This contrast made the tumor edge easier to see than on conventional structural imaging from the same optical system, suggesting that C‑OCE could one day guide surgeons to remove all cancer while avoiding unnecessary sacrifice of blood vessels and healthy pancreas. 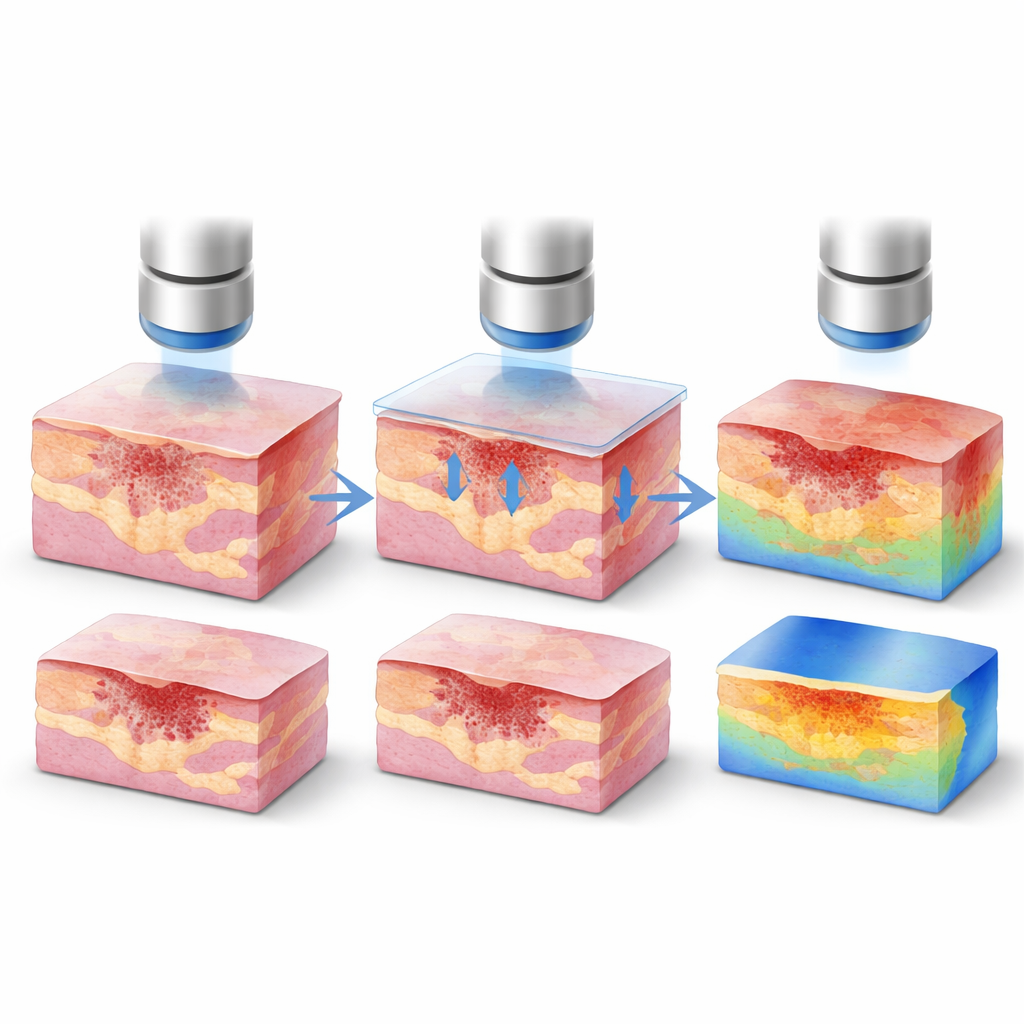
What this could mean for future operations
Overall, the study shows that a compact, light‑based scanner can objectively measure how stiff different parts of the pancreas are during surgery, mapping out healthy, scarred, and cancerous regions in a way that correlates well with full laboratory histology. Compared with relying on touch alone, this approach could more reliably flag patients at high risk of fistula, help identify pancreas segments rich in transplantable islets, and sharpen the line between tumor and normal tissue. While further development and clinical trials are needed before such devices are used routinely in operating rooms, this work points toward a future in which surgeons see not just what the pancreas looks like, but how it feels—quantitatively—at every point they need to cut.
Citation: Gubarkova, E., Potapov, A., Vasilchikova, E. et al. Identifying intact and fibrotic parenchyma in pancreatic ductal adenocarcinomas using compression optical coherence elastography. Sci Rep 16, 13078 (2026). https://doi.org/10.1038/s41598-026-40746-6
Keywords: pancreatic cancer, tissue stiffness imaging, intraoperative imaging, postoperative pancreatic fistula, islet transplantation