Clear Sky Science · en
Clinical outcomes of directional atherectomy versus plain balloon angioplasty as vessel preparation prior to drug-coated balloon treatment for femoropopliteal occlusive disease
Why clearing leg arteries matters
As people live longer and conditions like diabetes and high blood pressure become more common, many develop clogged arteries in their legs. This can cause pain while walking, slow-healing wounds, and in severe cases, the risk of losing a foot or leg. Doctors now often treat these blockages from the inside with tiny balloons and other tools, hoping to restore blood flow without leaving permanent metal tubes, or stents, behind. This study asks a practical question: when preparing these narrowed leg arteries for a special drug-coated balloon, is it really worth using a more complex plaque-removal device, or is a simple balloon good enough?
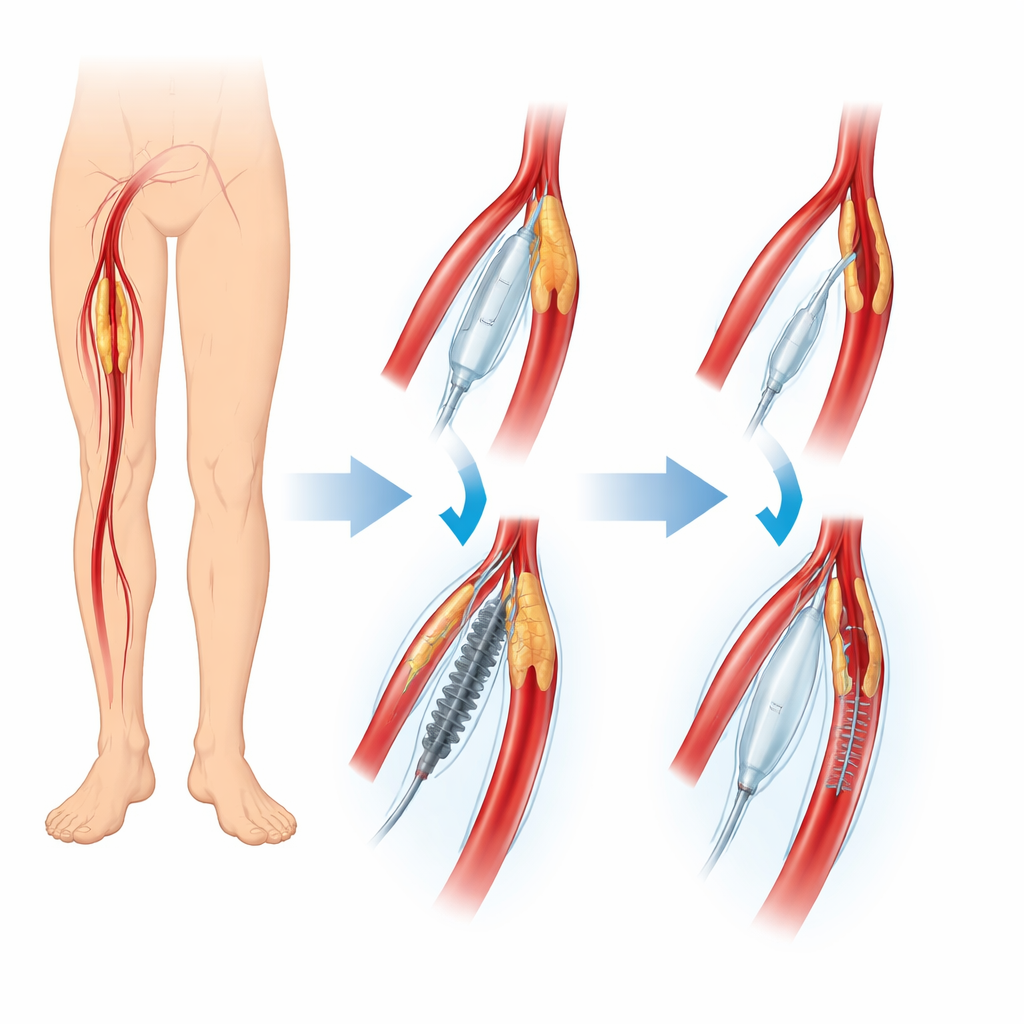
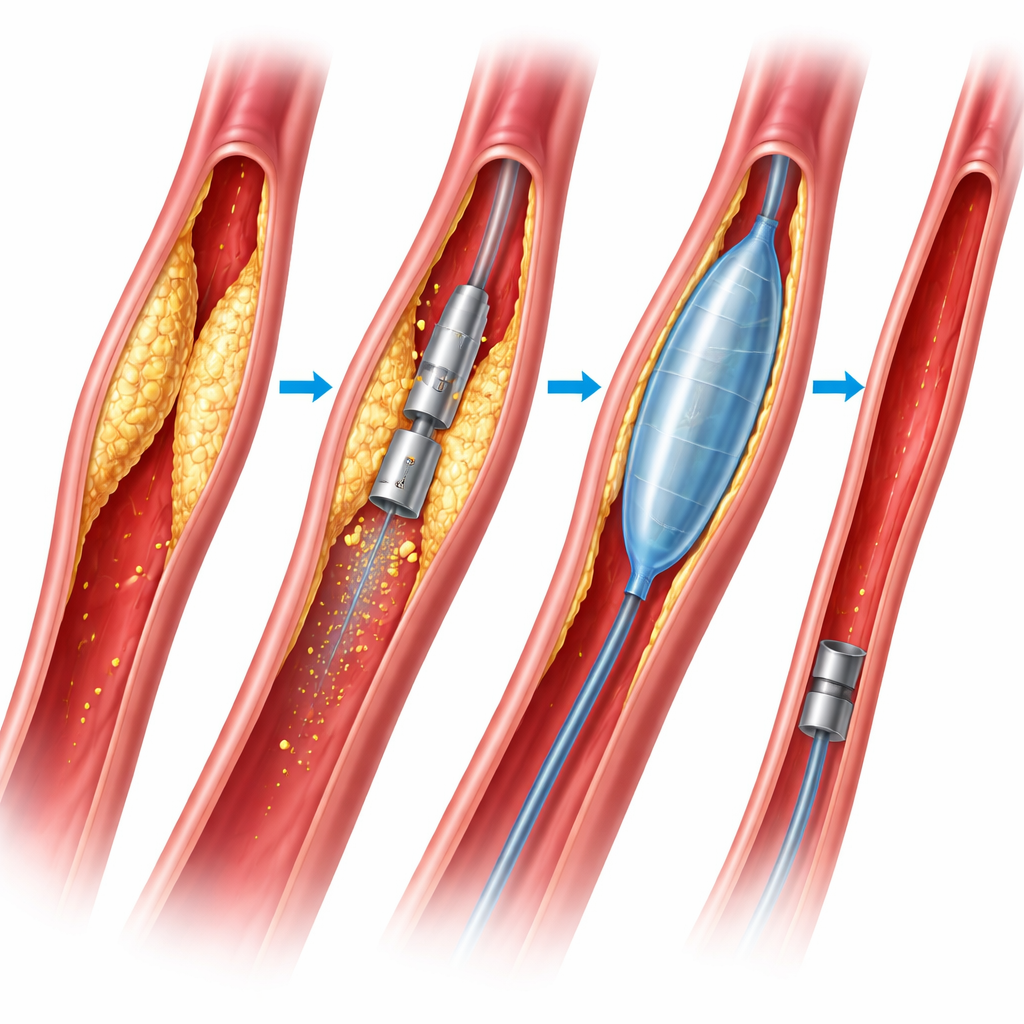
Two ways to open a clogged leg artery
The research focused on people with femoropopliteal disease, a common form of artery blockage in the thigh and behind the knee. All patients were treated in hospitals across China and enrolled in a large ongoing registry that tracks real-world outcomes. Everyone received a drug-coated balloon, which delivers medicine to the artery wall to help keep it open. Before that, however, doctors prepared the blocked vessel in one of two ways. Some patients were treated with a simple uncoated balloon that is inflated to stretch the blockage. Others received a directional atherectomy device, a small cutting tool that shaves off plaque from inside the artery, followed by the same type of drug-coated balloon.
How the study was set up
Because this was not a randomized trial, the investigators used detailed statistical matching to make the two groups as similar as possible. From more than 1,200 eligible patients, they created a carefully balanced comparison between 147 people treated with plaque removal and 480 treated with balloon stretching alone. These patients had similar ages, risk factors such as smoking and diabetes, and similar types of blockages. The team then followed them for up to two years, tracking not only what happened in the operating room but also longer-term events such as repeat procedures, major amputations, and deaths.
What happened in the operating room
Inside the procedure suite, the plaque-removal strategy changed how the operations looked, but not how long they took. When doctors used atherectomy, they needed to place stents far less often, and when stents were used they tended to be shorter. The treated artery could also accept a slightly larger drug-coated balloon, suggesting a more thoroughly opened channel. On the other hand, this technique was more expensive and led to more minor issues such as small clots or minor bleeding at the access site. Serious complications were rare and occurred at similar rates in both groups. Overall, both methods quickly improved blood flow and leg symptoms to a similar degree when measured by standard clinical scores.
How patients fared over two years
Over about two years of follow-up, the two strategies produced almost identical results where it matters most to patients. Survival rates were similar. The need for repeat treatment in the same artery segment did not differ, nor did the chances of keeping the limb without major amputation. When the researchers looked at specific groups of patients, one pattern stood out: people whose arteries were completely blocked from end to end, rather than just narrowed, seemed to benefit more from plaque removal in terms of avoiding stents. For other lesion types, such as shorter blockages or varying degrees of calcium buildup, the advantage of atherectomy was less clear.
What this means for people with leg artery disease
For patients and clinicians, the message is nuanced but reassuring. Using a plaque-removal device before a drug-coated balloon can help doctors rely less on permanent metal stents, especially in very tough, fully blocked segments, without sacrificing safety or long-term results. However, this benefit comes with extra cost and a slightly higher rate of minor complications, and it does not appear to improve survival or reduce repeat procedures overall compared with careful use of standard balloons. The authors suggest that this tool should be used selectively in the most complex blockages, rather than as a one-size-fits-all solution for every narrowed leg artery.
Citation: Wang, X., Ye, M., He, C. et al. Clinical outcomes of directional atherectomy versus plain balloon angioplasty as vessel preparation prior to drug-coated balloon treatment for femoropopliteal occlusive disease. Sci Rep 16, 14119 (2026). https://doi.org/10.1038/s41598-026-40423-8
Keywords: peripheral artery disease, leg artery blockage, drug-coated balloon, atherectomy, stent use