Clear Sky Science · en
A handheld near infrared scanner for the detection of acute traumatic intracranial hemorrhage
Why a Pocket Brain Scan Matters
When someone hits their head in a car crash, on the playing field, or in a fall, the most dangerous damage is often hidden. Bleeding inside the skull can quickly become life-threatening, yet the standard way to find it—a CT scan—usually exists only in larger hospitals. This study tests a new handheld scanner that uses invisible near-infrared light to quickly check for dangerous brain bleeding at the scene, in an ambulance, or in small clinics, without radiation or bulky machines. 
A New Kind of Head Check
The device, called the Archeoptix NIRD scanner, looks more like a thick computer mouse than a hospital machine. A caregiver places it against the scalp and sweeps it across the head in a series of passes guided by a laptop screen. Before scanning, they briefly hold the device on an area with little or no hair, such as the forehead or shoulder, so the system can adjust for skin tone. During each pass, the scanner shines a single color of near-infrared light—just beyond what our eyes can see—into the head and measures how much light comes back from shallow tissues, like scalp and skull, and from deeper structures, like brain and any pooled blood.
How Light Reveals Hidden Bleeding
Blood strongly absorbs near-infrared light, so a pocket of fresh bleeding inside the skull will weaken the signal detected from deeper tissues. The device compares the light detected by two pairs of sensors: one closer to the light source, which mainly sees surface tissues, and one farther away, which sees deeper tissues. By taking the ratio between these signals thousands of times per second, the system can tell whether something deep inside is soaking up extra light. In healthy brain tissue, this ratio falls in a typical range; when it drops below a preset cutoff, the system flags a likely bleed of at least about three teaspoons in volume lying within roughly a finger’s width and a half from the scalp. The processed data are then mapped onto a three-dimensional model of a head to show where the bleeding probably lies. 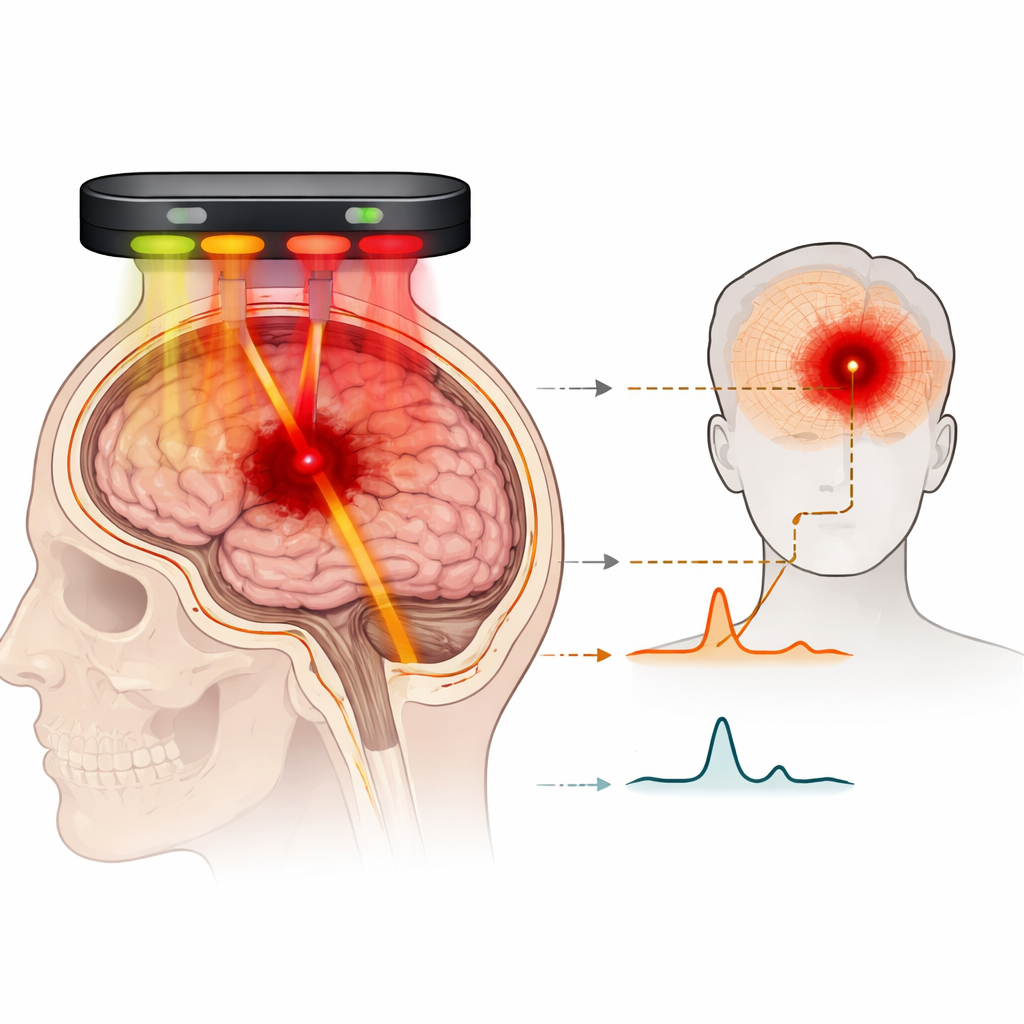
Putting the Scanner to the Test
To see how well this works in real patients, the researchers scanned 37 people who had traumatic brain injuries and CT-confirmed bleeding inside the skull, along with 40 healthy volunteers who had no history of head injury. All patients with bleeding were scanned within about a day of their trauma; most had common types of surface bleeding such as subdural or epidural hematomas. Independent reviewers, who did not know the CT results, inspected each scan and simply judged whether bleeding was present and whether its location matched the CT image. They correctly identified bleeding in all 37 injured patients and correctly found no bleeding in all 40 healthy controls. In 35 of the 37 injured patients, the scanner’s indicated bleed location agreed with the CT scan; the two mismatches were traced back to the operator not following the recommended scanning pattern.
Learning to Use the Tool Well
The study also examined how people actually used the device. Because injured patients were lying on their backs and sometimes wearing neck collars, operators had to shorten some scan paths to avoid painful injuries or awkward head positions. The system occasionally reported problems such as outside light leaking into the sensor shroud or the device lifting slightly off the scalp, which could distort the readings. These errors were more common when scanning injured patients and often forced operators to repeat passes. Interestingly, the data showed that very quick passes tended to cause one kind of error, while overly slow, hesitant passes favored another, suggesting that training users to keep steady pressure and a smooth pace can improve both speed and accuracy. Reported side effects were minimal—some subjects noted mild discomfort, and no skin damage occurred.
Promise and Limits for Real-World Use
Although the pilot study is small, the results suggest that this portable scanner can reliably detect moderate-sized, relatively shallow brain bleeds after trauma, while correctly reassuring when no such bleed is present. It cannot yet be relied on to find very small or deep bleeds, and it may be less accurate in older people whose brains have shrunk away from the skull, or in cases of long-standing, partially broken-down blood. Larger, carefully blinded studies are needed to pin down its true sensitivity and specificity and to test it in ambulances, rural clinics, and busy emergency departments. Still, for first responders and remote health workers who currently must guess who urgently needs a CT scan, this kind of pocket-sized brain-checking tool could one day make the difference between early life-saving treatment and a dangerous delay.
Citation: D’Amario, S., Bougadis, J., Coverdale, N.S. et al. A handheld near infrared scanner for the detection of acute traumatic intracranial hemorrhage. Sci Rep 16, 12330 (2026). https://doi.org/10.1038/s41598-026-38268-2
Keywords: brain bleed, head injury, near infrared scanning, emergency triage, portable diagnostics