Clear Sky Science · en
Route-dependent dissemination with conserved blood–tumor barrier ultrastructure in intracranial metastasis models
Why this matters for people with cancer
When cancers spread to the brain, they become far harder to treat. Many drugs that work elsewhere in the body cannot easily cross the brain’s natural defenses. This study asks a deceptively simple question with big implications: does it matter how cancer cells first reach the brain, or does the brain itself ultimately reshape the battle in the same way every time? By comparing two common experimental models, the authors show that while the visible pattern of brain tumors can differ, the fine-scale damage to the brain’s protective blood barrier converges on a shared, stereotyped failure mode. 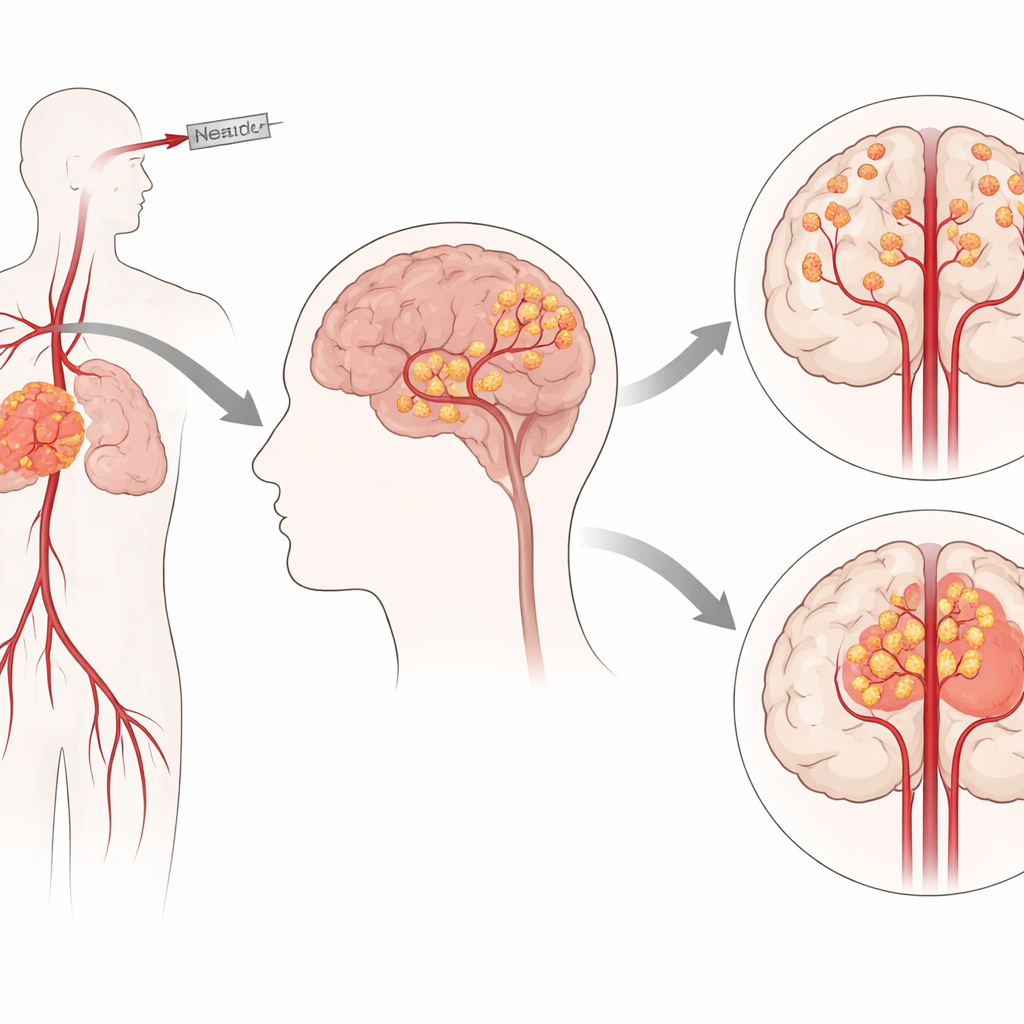
The brain’s protective gatekeeper
The brain is protected by a highly selective filter often called the blood–brain barrier. Rather than a simple wall, it is a living community of cells: the inner lining of blood vessels, supporting cells wrapped around them, and nearby nerve cells all cooperate to tightly control what enters brain tissue. In healthy conditions this system keeps the environment around brain cells stable, allowing precise electrical signaling. In brain metastasis, however, invading tumor cells must either slip through this barrier or hijack it. They tend to cling to existing blood vessels and their surrounding scaffolding, using this structure as “soil” in which to take root and grow.
Two ways cancer cells are sent to the brain
To study these events, researchers use mouse models that introduce tumor cells into the brain in different ways. One approach injects cells directly into the brain, creating a single, well-defined mass but also causing local injury and immediate disruption of the barrier. Another approach injects cells into a major neck artery so they travel in the bloodstream and lodge in brain vessels more naturally. Standard versions of this blood-borne method are plagued by large tumors in the face and skull that obscure brain signals and complicate sampling. In this study, the team refined the arterial approach by tying off a side branch to reduce stray seeding outside the brain, then compared it directly to the precise brain injection method.
Different tumor patterns, similar overall fate
The refined arterial method produced many small and medium-sized tumor spots scattered across both sides of the brain, better mimicking the multifocal spread seen in patients. The direct injection method, by contrast, yielded a single large mass at the injection site, with some artifactual spread along the needle track. When the researchers followed tumor growth over time using light-emitting cancer cells, the two models showed clearly different growth curves: the scattered tumors and the single mass expanded at different rates. Yet when they looked at how long the animals survived under preset humane rules, there was no statistically clear difference between groups at the sizes studied, suggesting that both patterns can be similarly deadly even though they look very different on scans. 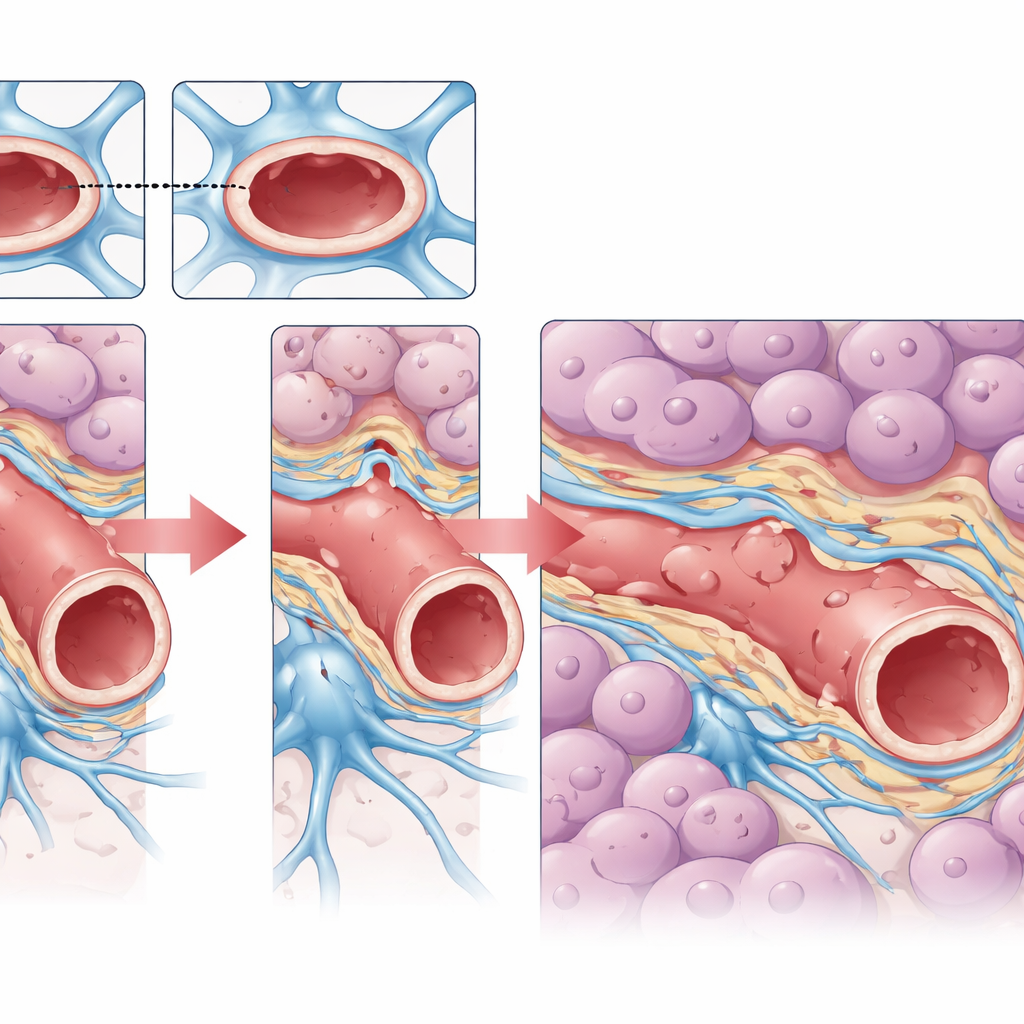
Inside the damaged microscopic barrier
The most striking findings came from zooming in with electron microscopes on the border where tumor meets brain. Here, the authors examined the ultrastructure of tiny vessels in melanoma brain metastases formed by either the blood-borne or direct injection route. Despite their very different beginnings and macroscopic shapes, the vessels in both models showed the same hallmarks of failure. The vessel-lining cells were swollen and full of bubble-like pockets, hinting at abnormal transport activity. The normally smooth supporting layer around the vessel was thinned and broken. The star-shaped brain support cells that usually wrap the vessel had pulled back, leaving abnormal spaces. Together these changes point to a common pattern of breakdown in the brain’s vascular unit once a metastasis has fully taken hold.
What this may mean for treatment
These observations support a unifying idea: no matter how cancer cells first arrive in the brain, established metastases may push the local blood–brain barrier toward a similar, less mature and more leaky state. This helps explain why imaging in patients often shows patchy regions of contrast uptake, reflecting areas where the barrier has remodeled to different degrees. It also highlights why model choice matters for drug testing. The single-mass model is well suited for studying therapies against large, highly leaky tumors, while the multifocal arterial model captures the mix of tiny, still-protected spots and larger lesions that clinicians face. By showing that the microscopic pattern of barrier damage is conserved, this work offers a clearer conceptual map for linking vessel structure, imaging signals, and drug response—and sets the stage for more quantitative studies that could guide better treatments for people with brain metastases.
Citation: Zhao, J., Zhang, Y., Wei, Z. et al. Route-dependent dissemination with conserved blood–tumor barrier ultrastructure in intracranial metastasis models. Sci Rep 16, 13508 (2026). https://doi.org/10.1038/s41598-026-37760-z
Keywords: brain metastasis, blood-brain barrier, neurovascular unit, animal models, cancer drug delivery