Clear Sky Science · en
Proteomic risk score for early prediction of kidney disease progression in individuals with APOL1 high-risk genotypes
Why this research matters
Kidney failure is a silent threat that often strikes without warning, especially in people of African ancestry who carry certain inherited variants of a gene called APOL1. Many of these individuals live for years with normal test results, only to develop severe kidney problems later. This study introduces a new blood-based risk score that aims to spot who is most likely to get into trouble long before traditional tests sound the alarm, opening the door to earlier and more targeted care.
The hidden burden of kidney failure
Chronic kidney disease affects hundreds of millions of people worldwide and, when it progresses to kidney failure, patients need dialysis or a transplant to survive. In the United States, people of African ancestry develop kidney failure at nearly four times the rate of those of European ancestry. Part of this gap comes from social and economic factors, but genetics also play a strong role. Variants in APOL1 sharply increase the chance of kidney failure, yet most carriers never develop disease. That uncertainty creates a major problem: doctors know a patient is at higher genetic risk but cannot tell whether they are one of the few who will progress or one of the many who will not.
Looking beyond routine kidney tests
Standard tools, such as measuring how well the kidneys filter blood (eGFR) and how much protein leaks into the urine, work best once damage is already established. A widely used equation, the Kidney Failure Risk Equation, is fairly accurate only in people whose kidney function is already reduced. Genetic risk scores capture inherited risk but are static and have limited predictive power across diverse populations. The researchers behind this study turned to plasma proteomics, a technology that measures thousands of proteins in a blood sample at once. Because proteins reflect real-time biology, they can reveal early tissue injury that routine tests miss.
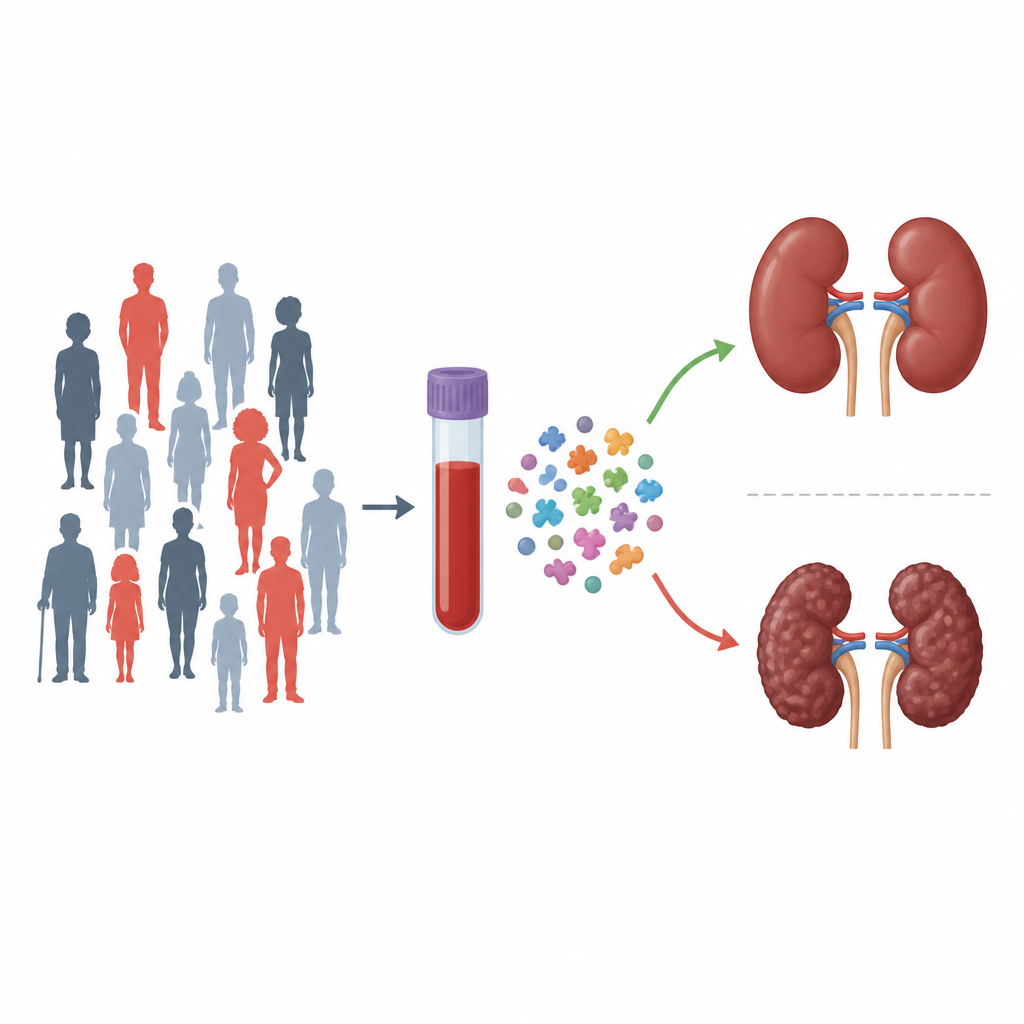
Building a blood protein risk score
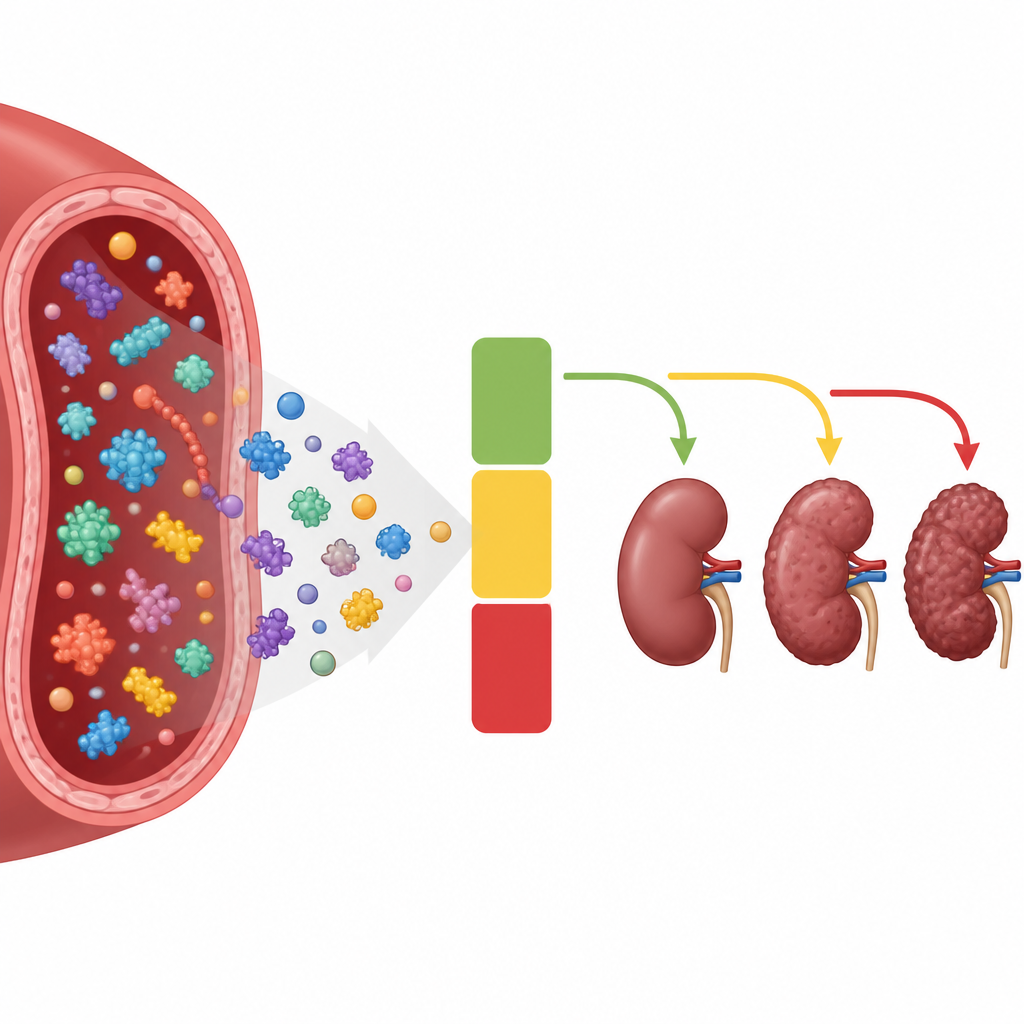
The team analyzed blood samples from 1,113 participants of African ancestry in the Penn Medicine BioBank who carried APOL1 high-risk genotypes. They focused on 851 people whose kidney function still appeared normal. Using a sophisticated statistical approach, they sifted through more than 7,000 measured protein forms and identified a set of nine proteins that, together with age, sex, kidney function and urine protein, best forecasted serious events such as large drops in kidney function, need for dialysis or transplant, or death. This combination was turned into the APOL1 Proteomic Risk Score, or APRS. People in the highest APRS group had about a 63 percent chance of one of these events over ten years, compared with just over 3 percent in the lowest group.
Testing the score in different groups
To see if APRS would hold up outside the original hospital system, the researchers tested it in two large community studies: the Atherosclerosis Risk in Communities study and the UK Biobank. In both groups, APRS accurately separated those who would go on to have kidney problems or die from those who would remain stable, even though participants lived in different regions and health systems. Across these and other comparison groups, APRS consistently outperformed the standard clinical equation and genetic risk scores, especially in people whose kidney function still looked normal. The blood proteins that make up APRS were also linked to scarring and injury in kidney tissue samples, lending biological support to the idea that the score is capturing real early damage.
What this could mean for patients
APRS is not a treatment, but it could change when and how treatment is offered. By identifying high-risk APOL1 carriers long before standard tests detect trouble, doctors could monitor these individuals more closely and, as new APOL1-targeted drugs like inaxaplin become available, focus those therapies on the patients most likely to benefit. Modeling suggests that using APRS to select candidates for such a drug could nearly halve the number of people who need to be treated to prevent one bad outcome. Low scores could also reassure many carriers that their personal risk is small, although regular medical follow-up would still be essential.
The takeaway for non-specialists
This study shows that a detailed snapshot of proteins in a single blood sample can turn broad genetic risk into a clear, individualized forecast for future kidney health in APOL1 high-risk individuals. While more work is needed before the test becomes part of everyday care, APRS provides a practical framework for earlier, more precise intervention. In the long run, it may help reduce the unequal burden of kidney failure among people of African ancestry by ensuring that the right people receive the right care at the right time.
Citation: Li, C., Richards, S.M., Quinn, G. et al. Proteomic risk score for early prediction of kidney disease progression in individuals with APOL1 high-risk genotypes. Nat Med 32, 1701–1707 (2026). https://doi.org/10.1038/s41591-026-04337-2
Keywords: kidney disease, APOL1, proteomics, risk prediction, health disparities