Clear Sky Science · en
Integrated epidemiological and molecular data inform the relationship between precancer and cancer states of esophageal adenocarcinoma
Why this matters for people with heartburn
Esophageal adenocarcinoma is a deadly cancer that often begins with long-standing heartburn and damage to the lower esophagus. Doctors have long suspected that a condition called Barrett’s esophagus, where the normal lining is replaced by intestine-like cells, is the main warning stage. But about half of people with this cancer have no clear sign of Barrett’s at diagnosis, raising a worrying question: can this cancer arise out of the blue, or is Barrett’s simply hidden from view? This study tackles that question using large-scale patient data and modern genetic tools.
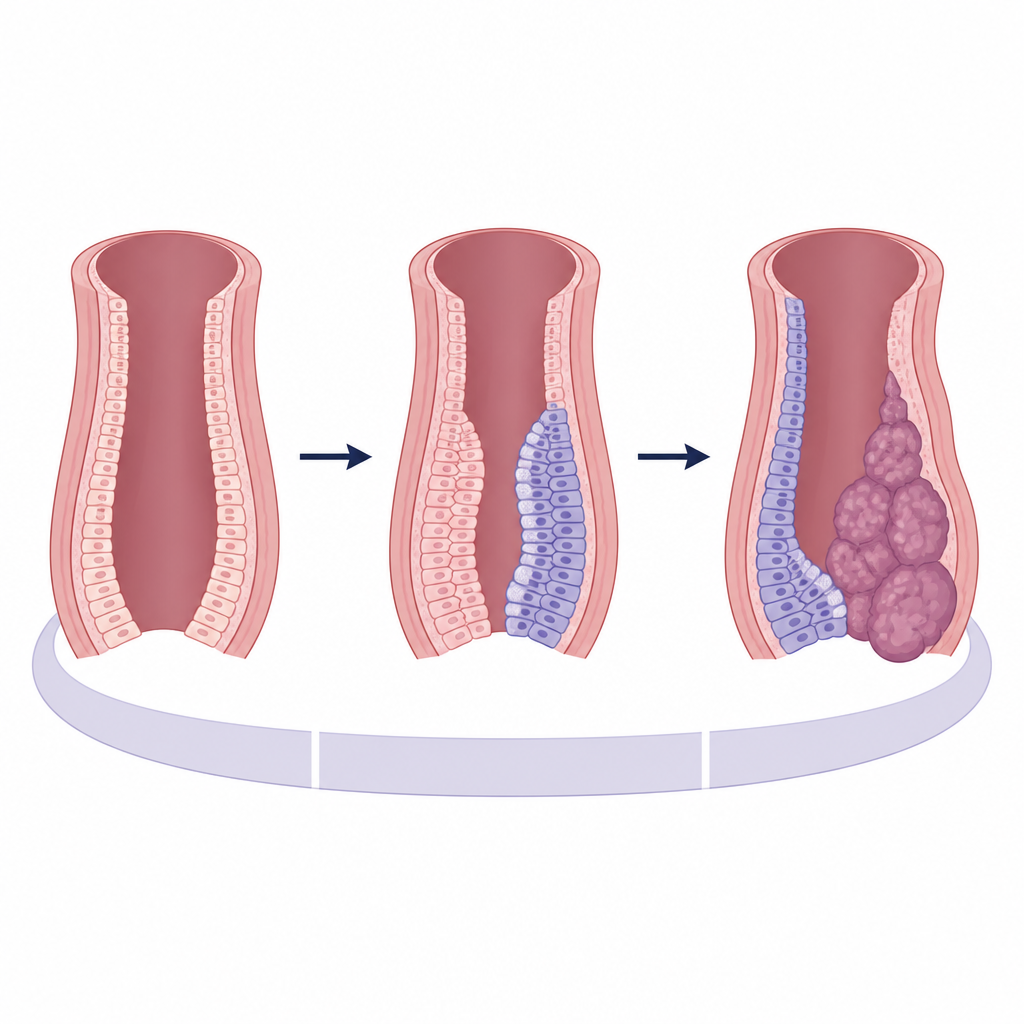
One suspected pathway, two apparent cancer types
The researchers focused on more than 3,100 people in the United Kingdom who had surgery or curative treatment for esophageal adenocarcinoma. Each case was carefully reviewed by specialists to decide whether visible or microscopic Barrett’s tissue was present next to the tumor. Patients were grouped as Barrett’s-positive, Barrett’s-negative, or uncertain. At the same time, the team collected detailed information about age, sex, weight, smoking, heartburn symptoms, medications and tumor stage. This set the stage to test whether cancers with and without visible Barrett’s really represent different diseases, or just different snapshots along the same route.
Risk factors look more alike than different
When the team compared basic characteristics, they found that people in both groups shared the classic risk profile for this cancer: mostly older, white men with a history of heartburn and often extra body weight. Some small differences appeared at first glance, such as slightly more obesity in the Barrett’s-positive group and a hint that smokers were more common in the Barrett’s-negative group. However, when the researchers used statistical models that accounted for multiple factors at once, these differences shrank and were no longer strong enough to clearly separate the two groups. The one consistent exception was tumor stage: cancers without visible Barrett’s were more often diagnosed at a later, more advanced stage.
The DNA story points to a shared origin
To look deeper, the team sequenced the complete DNA of tumors from 710 patients and compared them with 388 samples of Barrett’s tissue from patients who did not yet have cancer. They also performed more focused sequencing in 380 tumor regions from 87 patients to reconstruct how each cancer evolved over time. In Barrett’s tissue, they identified a set of genes and mutation patterns that seem to fuel early growth. Strikingly, these same genetic hallmarks appeared at similar frequencies in both Barrett’s-positive and Barrett’s-negative cancers. Measures of overall mutation load, large-scale DNA rearrangements and catastrophic chromosome shattering events were also nearly identical across the two cancer groups.
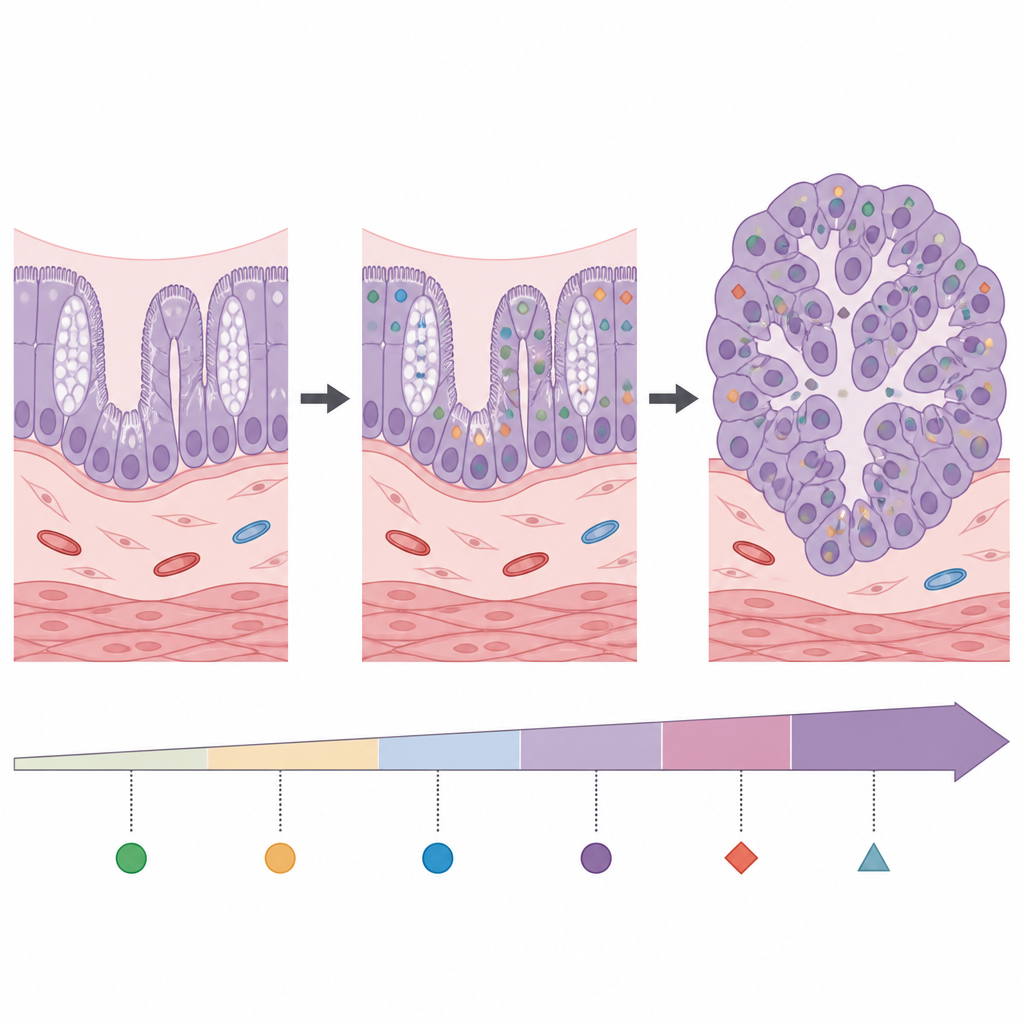
Invisible Barrett’s leaves a molecular fingerprint
Even when Barrett’s tissue cannot be seen around a tumor, it may leave a molecular fingerprint. Using high-resolution spatial transcriptomics, which maps gene activity across thin tissue slices, the researchers showed that many cancer cells in both groups still express genes typical of intestinal-type Barrett’s lining. In contrast, cancer-specific genes were not active in benign Barrett’s areas except where high-grade precancerous change was present. Protein staining confirmed that key Barrett’s markers, such as TFF3 and REG4, are often present inside tumor cells, including in some cancers labeled Barrett’s-negative. Together with clinical data showing that some patients lost visible Barrett’s between earlier endoscopies and later cancer surgery, this supports the idea that expanding tumor growth can simply overrun and obscure its Barrett’s starting point.
What this means for early detection and care
Overall, the study finds little evidence for a separate, Barrett’s-independent route to esophageal adenocarcinoma. Instead, the data support a single main pathway in which intestinal-type changes in the lower esophagus set the stage for cancer, even if that altered tissue is no longer visible once the tumor is advanced. For patients and health systems, this strengthens the case for finding better, less invasive ways to detect Barrett’s-like changes and to identify which of these are truly at high risk of turning into cancer. While it remains uncertain whether broad screening will lower deaths, recognizing Barrett’s as the common starting point can help refine prevention, monitoring and research efforts aimed at catching this cancer earlier.
Citation: Zamani, S.A., Wu, L., Black, E.L. et al. Integrated epidemiological and molecular data inform the relationship between precancer and cancer states of esophageal adenocarcinoma. Nat Med 32, 1805–1816 (2026). https://doi.org/10.1038/s41591-026-04331-8
Keywords: esophageal adenocarcinoma, Barrett’s esophagus, cancer precursors, early cancer detection, genomic profiling