Clear Sky Science · en
Interpretable and granular video-based quantification of motor characteristics from the finger-tapping test in Parkinson’s disease
Why Tapping Fingers Can Reveal Brain Health
For many people with Parkinson’s disease, everyday movements like buttoning a shirt or typing on a keyboard gradually become slower and smaller. Doctors often assess these changes with a simple finger-tapping test: patients rapidly touch their thumb and index finger together. Traditionally, a clinician watches and assigns a single score. This study shows how ordinary video recordings and artificial intelligence can turn that brief test into a rich, objective readout of movement problems, potentially making Parkinson’s monitoring more precise and easier to perform at home.
A Simple Test with Hidden Complexity
The finger-tapping task looks straightforward, but specialists know it contains several distinct problems rolled into one. People with Parkinson’s may show reduced movement size (hypokinesia), slower motion (bradykinesia), a gradual decline in performance over a few seconds (known as a sequence effect), and irregular pauses or hesitations (hesitation-halts). Until now, these patterns were mostly judged by eye and collapsed into a single severity score, which can vary from one clinician to the next. The authors set out to break this test apart, measuring each of these four movement issues separately using only video.
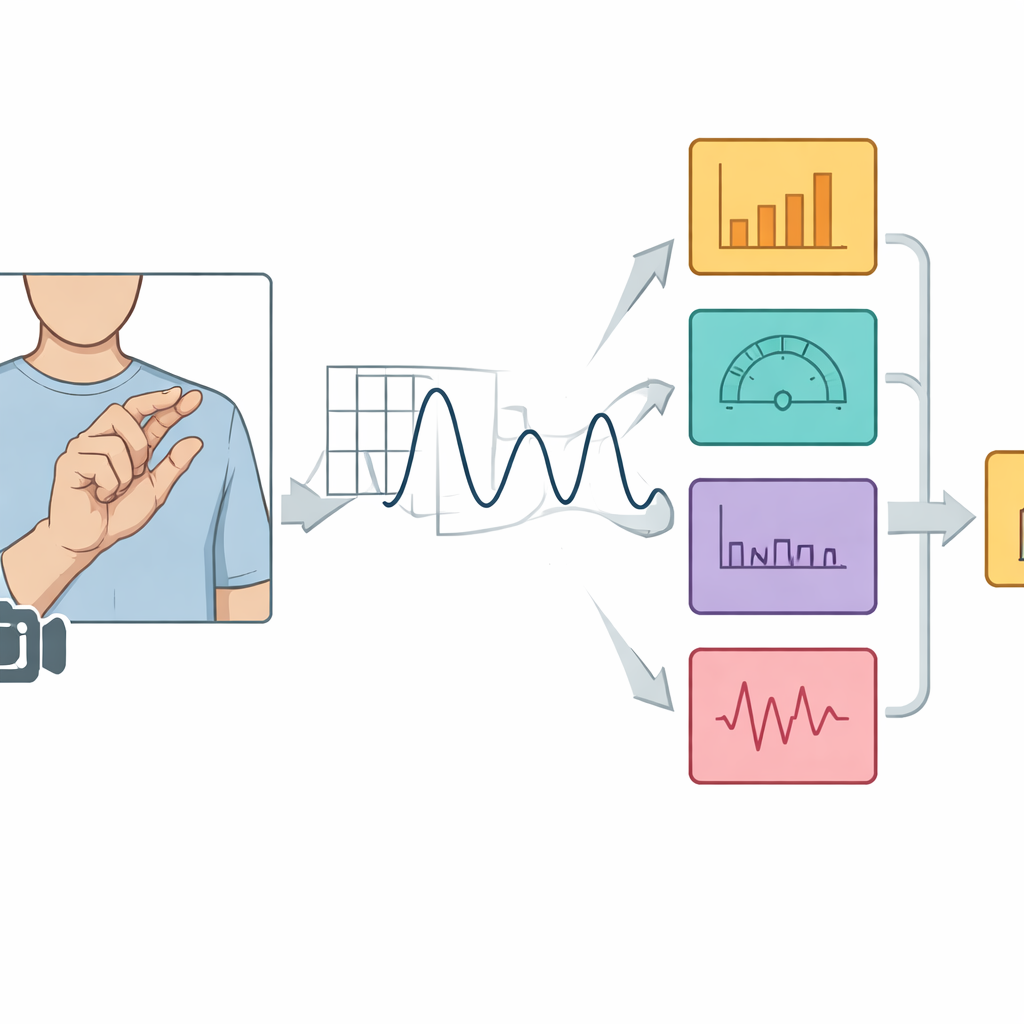
Turning Video of Hands into Numbers
The researchers analyzed more than 4,000 finger-tapping videos from 446 people with Parkinson’s who took part in the Personalized Parkinson Project. Using computer vision software, they automatically located key points on the hand—such as the thumb tip, index finger tip, and wrist—in every frame. From these points, they calculated the changing distance between thumb and index finger as the person tapped. By also tracking the length of the palm, they scaled this distance so that the measurements would be comparable even when the camera angle or distance varied from one recording to another. The resulting wavelike signal of opening and closing fingers became the basis for all later calculations.
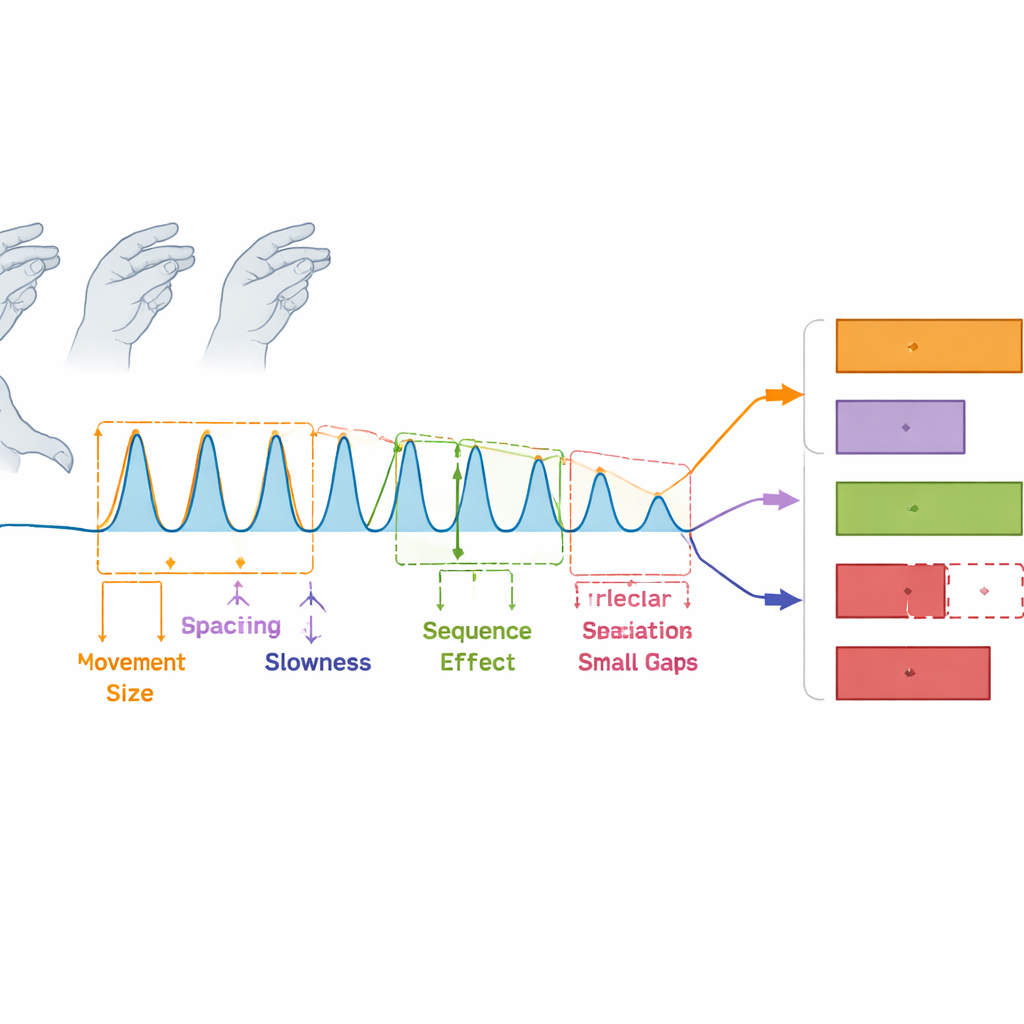
Measuring Four Kinds of Movement Problems
From each signal, the team built a compact set of 12 features designed to line up with the four clinically defined movement problems. Average tap height captured how widely the fingers opened, reflecting hypokinesia. The time between peaks in the signal captured how long each tap cycle took, reflecting bradykinesia. Two speed measures combined information about size and timing of the taps. Additional features tracked whether taps shrank or slowed over the short test (the sequence effect), and how much the size, timing and speed of taps fluctuated from one cycle to the next, including unusually long pauses that counted as interruptions (hesitation-halts). Statistical tests showed that most of these video-based measures worsened in step with the standard clinical score, especially for movement size, slowness and irregular pauses.
Revealing Finer Patterns in Parkinson’s Movement
To see how these measurements naturally grouped together, the authors used a statistical technique that clusters related features. The expected four movement domains did appear, but the data hinted at even finer structure. In particular, the sequence effect and hesitation-halts each seemed to split into two subtypes: one driven by changes in movement size and speed, and another driven by changes in timing and the presence of interruptions. This suggests that what looks like a single kind of problem at the bedside may actually consist of several distinct patterns, which could one day be linked to different brain changes or treatment responses.
From Objective Features to Practical Scoring
Because today’s gold standard is still the Movement Disorder Society’s Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), the researchers also asked whether their features could predict the usual finger-tapping severity scores. They trained several types of machine-learning models on the video features. The best model, a gradient-boosted decision-tree system, correctly placed recordings into mild, moderate, or severe categories more often than previous video-based methods. Importantly, the same approach also worked well on a separate dataset recorded with a different camera setup, suggesting it can generalize beyond a single lab or clinic.
What This Means for Patients and Care
In everyday terms, this work shows that a short video of someone tapping their fingers can be turned into a detailed, objective fingerprint of how Parkinson’s disease affects their movements. Instead of a single, subjective score, doctors and researchers can see separate numbers for how small, how slow, how fatigable, and how irregular the movements are. Because the method relies only on a camera and interpretable measurements, it could be used for large clinical trials and, eventually, for remote checkups at home. Future studies will need to show how these video-based markers change with medication and over years of disease, but this framework marks an important step toward more precise and convenient monitoring of Parkinson’s symptoms.
Citation: Zarrat Ehsan, T., Tangermann, M., Güçlütürk, Y. et al. Interpretable and granular video-based quantification of motor characteristics from the finger-tapping test in Parkinson’s disease. npj Parkinsons Dis. 12, 101 (2026). https://doi.org/10.1038/s41531-026-01307-w
Keywords: Parkinson’s disease, finger tapping test, computer vision, remote motor assessment, digital biomarkers