Clear Sky Science · en
CXCR3 is associated with T-cell-induced heart damage in acute rheumatic fever
Why this matters for young hearts
Acute rheumatic fever is a complication that can follow a common strep throat infection, yet it remains a major cause of heart damage in children and young adults worldwide. This study explores how the body’s own immune system, especially certain white blood cells called T cells, may drive injury to the heart valves. By mapping these immune changes in the blood and in diseased heart tissue, the researchers highlight new ways doctors might one day diagnose rheumatic fever earlier and reduce lasting heart damage.
A common sore throat with uncommon consequences
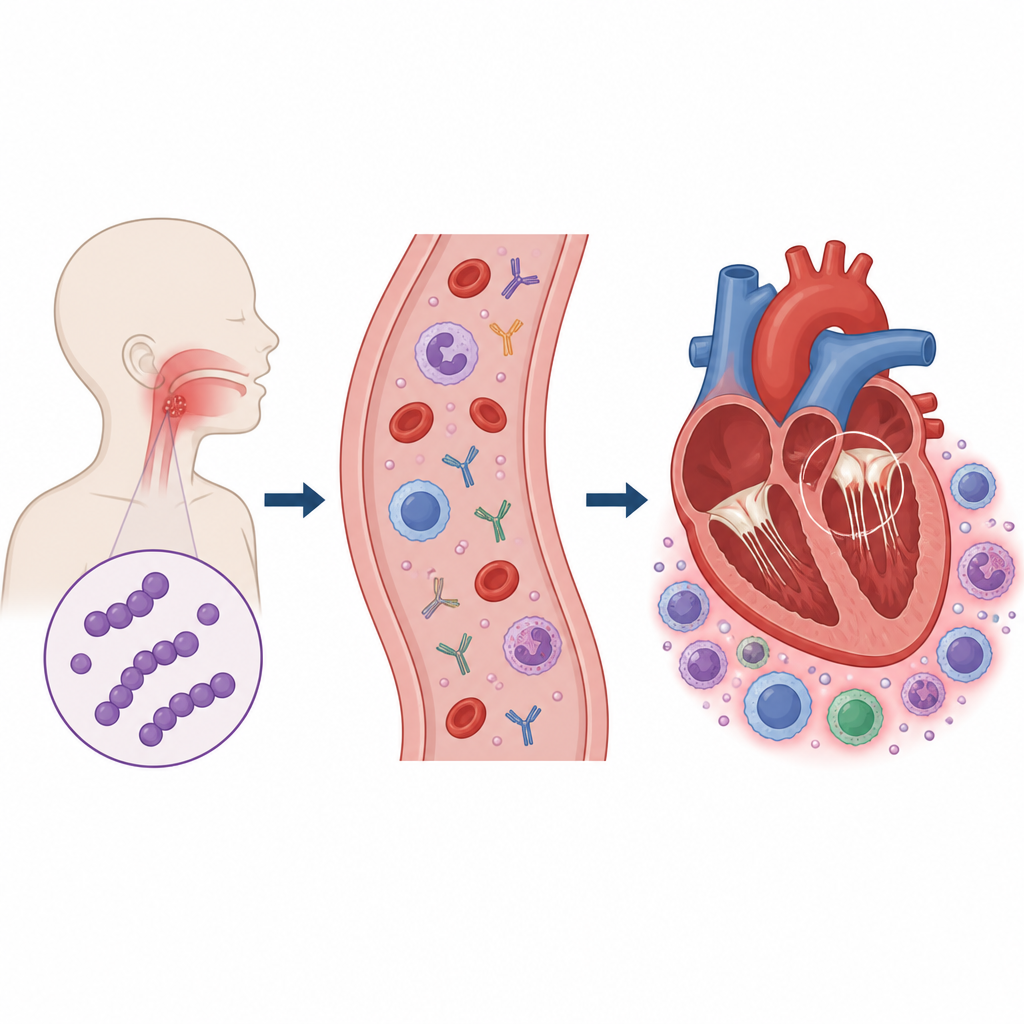
Acute rheumatic fever develops after infection with group A Streptococcus, the bacterium that causes strep throat. In some children, the immune system that once fought the germ begins to attack the body’s own tissues, especially the heart valves. This can lead to rheumatic heart disease, in which valves become scarred and leaky over time. The burden is greatest in low and middle income countries and among Indigenous and Pacific communities in Australia and Aotearoa New Zealand. Because there is no single blood test that confirms rheumatic fever, doctors rely on a set of clinical rules, and current treatments mainly prevent new infections rather than calming the runaway immune response itself.
Searching the blood for immune clues
The researchers analysed blood samples from children and young adults with definite rheumatic fever and compared them with several other groups, including patients with other serious infections or inflammatory illnesses, people with established rheumatic heart disease, and healthy volunteers. They measured many immune molecules in the blood, such as signaling proteins and antibodies, and used advanced cell analysis to profile circulating immune cells. Rheumatic fever showed a strongly inflamed pattern, with high levels of well known alarm signals like interleukin 6 and tumor necrosis factor, and an overall increase in helper T cells. But two features stood out as more specific: a rise in a chemical messenger called CCL5 and in a type of antibody known as IgG3, which together hinted at an immune response especially prone to causing tissue damage.
T cells on the move from blood to heart
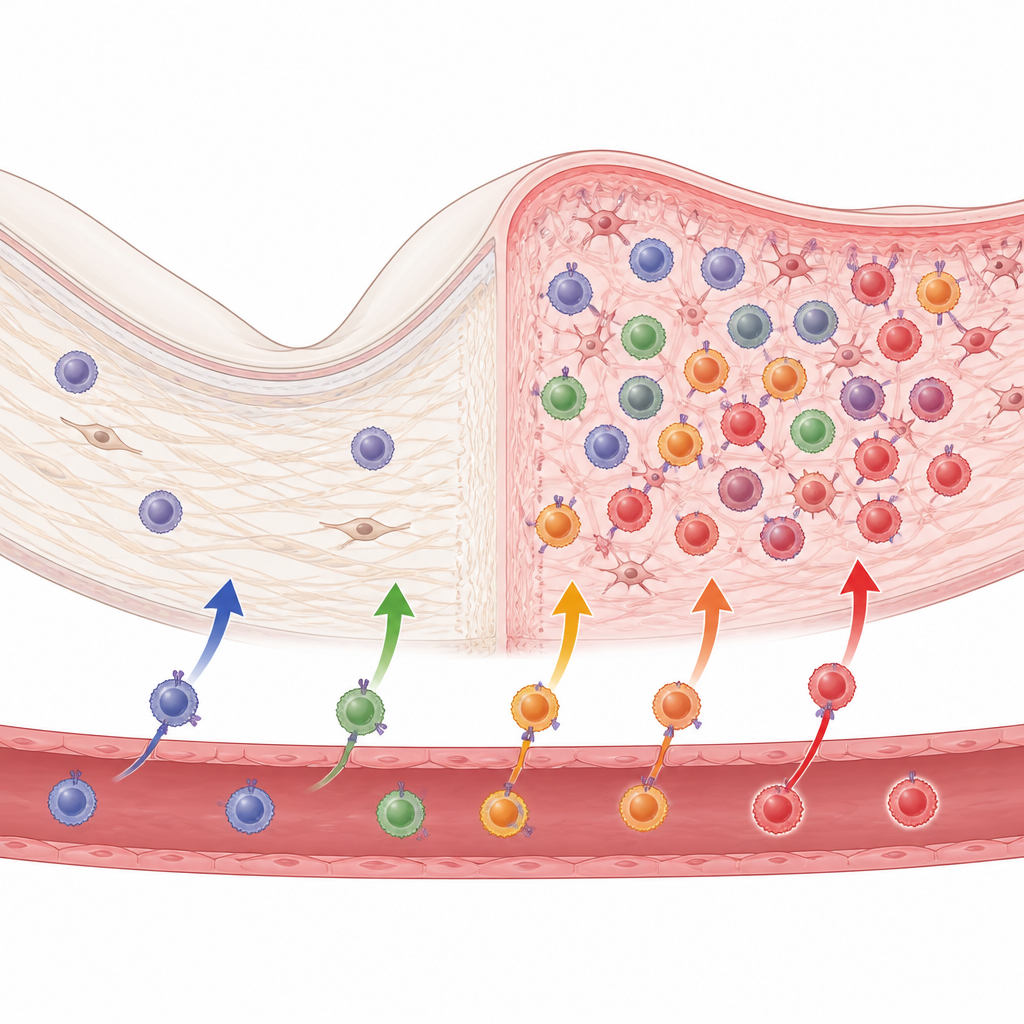
Looking more closely at immune cells, the team focused on T cells, which help coordinate and carry out attacks on perceived threats. They found that many types of T cells in rheumatic fever patients had reduced levels of a surface receptor called CXCR3, which normally guides these cells toward sites of inflammation. At first glance this drop in CXCR3 in the blood might suggest weaker immune activity. However, when the researchers examined diseased heart valves removed during surgery from children with rheumatic heart disease, they saw the opposite: these valves were packed with CXCR3 bearing T cells, especially in those with active, early stage disease. The findings point to a picture in which T cells that once circulated in the blood are drawn into the heart, leaving fewer CXCR3 marked T cells behind in the bloodstream.
A tilted balance in immune control
The study also uncovered a shortage of regulatory T cells, a subgroup that normally helps keep immune responses in check and prevents autoimmunity. At the same time, memory T cells that remember past threats were increased, suggesting a system primed for repeated attacks. When the scientists combined measurements of inflammation (C reactive protein), IgG3, CCL5, and the drop in CXCR3 on T cells, they could distinguish rheumatic fever from other conditions with high accuracy. This combined “immune fingerprint” supports a model in which strong inflammatory signals, damaging antibodies, and misdirected T cells work together to harm heart tissue.
What this means for future care
For non specialists, the key message is that rheumatic fever is not just a lingering infection but an immune misfire that pulls aggressive T cells into the heart while weakening the body’s own braking system. By showing that CXCR3 positive T cells accumulate in damaged valves and that specific blood markers track this process, the study suggests several existing immune targeting drugs might be repurposed to help patients, such as medicines that block interleukin 6 or tone down overactive T cells. Although more long term studies are needed, these insights bring researchers closer to blood based tools that could flag rheumatic fever earlier and to treatments that not only prevent new strep infections but also protect young hearts from ongoing immune attack.
Citation: Middleton, F.M., McGregor, R., Lorenz, N. et al. CXCR3 is associated with T-cell-induced heart damage in acute rheumatic fever. Nat Commun 17, 4664 (2026). https://doi.org/10.1038/s41467-026-71094-8
Keywords: acute rheumatic fever, rheumatic heart disease, T cells, heart valve inflammation, autoimmune heart damage