Clear Sky Science · en
Post-treatment SIV control is associated with specific features of viral persistence before and after treatment interruption
Why stopping HIV drugs safely matters
People living with HIV usually need to take antiretroviral drugs for life, because the virus hides inside long‑lived cells and can surge back as soon as treatment stops. Yet a rare group can pause therapy and keep the virus under control on their own. This study uses a monkey model of HIV infection to ask what makes that possible, and whether there are warning signs—before and just after stopping drugs—that predict who will control the virus and who will not.
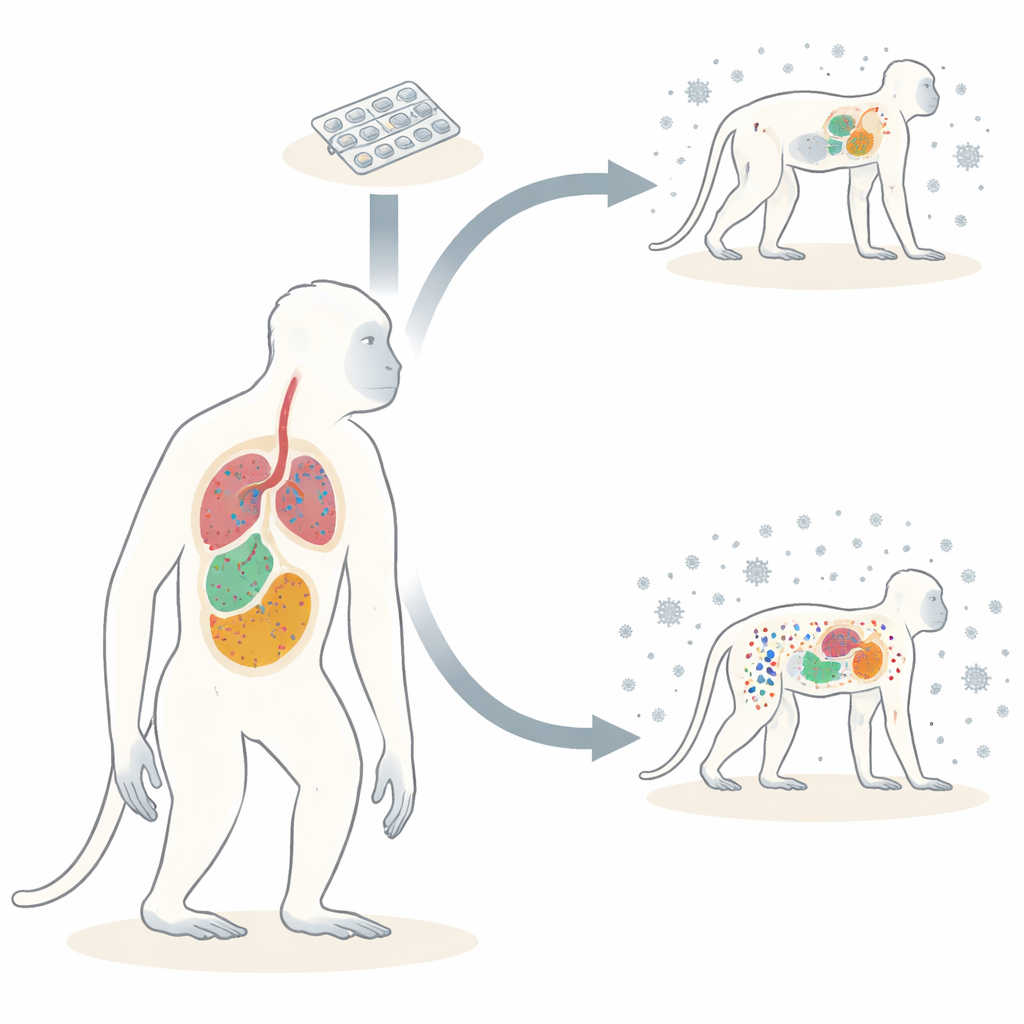
A monkey stand‑in for human infection
The researchers worked with cynomolgus macaques infected with SIV, a close cousin of HIV. All animals received the same strain of virus and standardized drug treatment, which began either four or 24 weeks after infection and lasted two years. Then, in most animals, treatment was deliberately interrupted to mimic what might happen in a future remission trial in people. Some macaques kept virus levels very low for many months after treatment interruption; these were called post‑treatment controllers. Others, the non‑controllers, experienced strong viral rebound similar to animals that had never been treated. Because the monkeys could be extensively sampled, the team measured virus in blood, many types of lymph nodes, gut, and other organs.
Hidden virus pockets across the body
HIV and SIV persist by integrating their genetic material into host cells, forming proviruses. Many of these proviruses are damaged, but a fraction remain intact and able to restart infection. The authors quantified total viral DNA, viral RNA (a sign of active copying), and the number of intact proviruses in dozens of tissues. Months after drugs were stopped, controllers showed strikingly low levels of viral DNA and RNA in blood, lymph nodes, gut, and several non‑lymphoid organs. Their viral burden looked similar to animals that had stayed on therapy continuously. Non‑controllers, in contrast, returned to viral levels and transcriptional activity comparable to untreated infection, indicating that rebounding virus had rapidly repopulated these reservoirs.
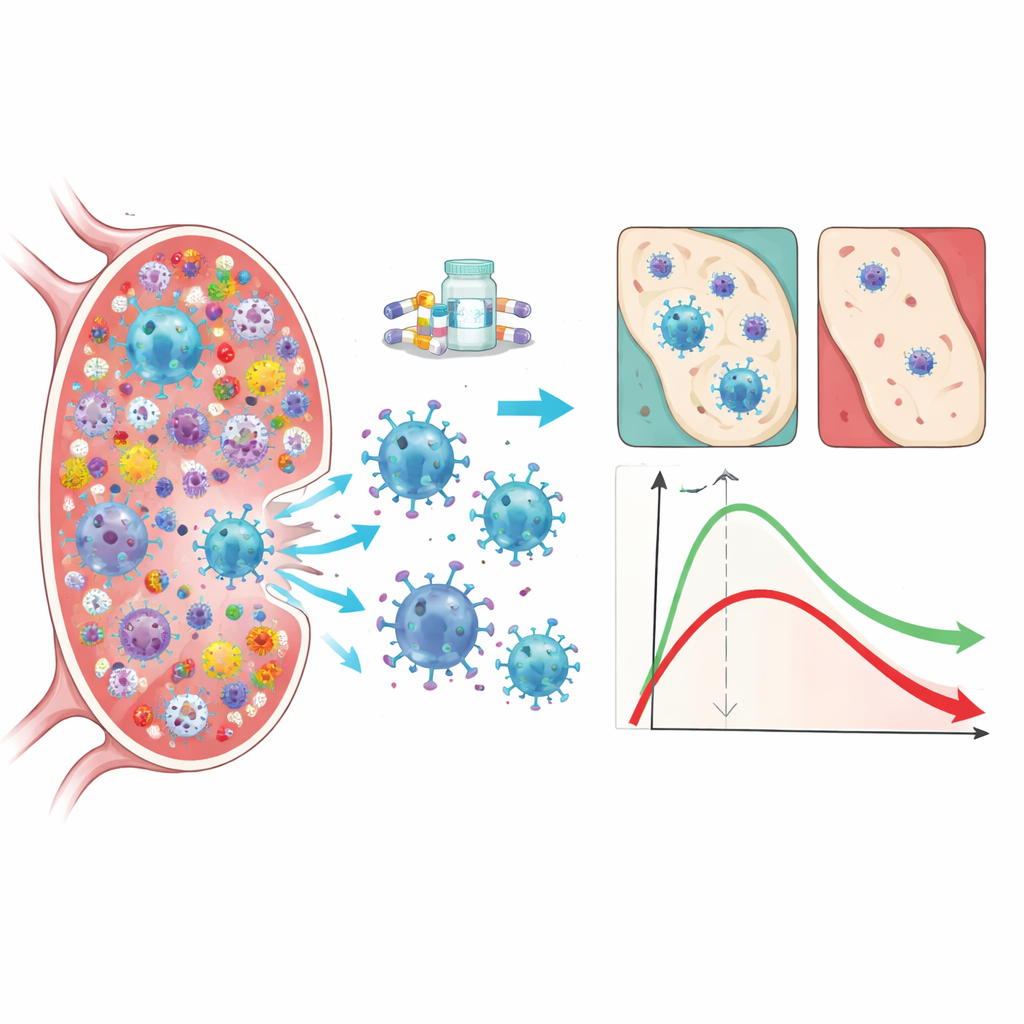
Early clues inside lymph nodes and blood
The most telling differences appeared in lymph nodes, where much of the immune response is organized. Even before treatment interruption, controllers already harbored fewer intact proviruses in peripheral lymph nodes than non‑controllers. The size of this intact reservoir predicted how much virus would circulate after drugs were stopped and what viral level would be seen at the end of follow‑up. These pre‑existing differences were linked to immune pressure: CD8 T cells from controllers—a type of killer immune cell—were better at suppressing SIV in laboratory tests, and stronger CD8 activity in lymph nodes correlated with fewer intact proviruses there. Importantly, a related signal could be captured from blood. Just seven days after stopping treatment, before viral rebound was detectable in plasma, non‑controllers already showed a rise in intact proviruses in blood cells, whereas controllers did not. These early blood measurements forecasted the scale of later rebound and mirrored what had been present in lymph nodes under therapy.
Immune cells that keep the lid on
Beyond simple counts of virus, the team examined the quality of the immune response. Controllers tended to have CD8 T cells with a stem‑like, long‑lived profile: they could proliferate, recirculate through lymphoid tissues, and were less exhausted or over‑activated. These cells were more multifunctional, able to perform several antiviral tasks at once, and showed strong capacity to suppress SIV in both blood and lymph nodes. Animals with this type of CD8 response had smaller reservoirs, lower viral transcription, and fewer intact proviruses across tissues. By contrast, non‑controllers showed more short‑lived effector cells and higher markers of chronic activation, a pattern associated with larger and more active viral reservoirs.
A virus held in check, not erased
Genetic sequencing of near‑full‑length viral genomes revealed that, in controllers, proviruses in tissues remained very similar to the original infecting strain and to viruses seen early in infection. This suggests little ongoing replication after treatment interruption. In non‑controllers, by contrast, tissue proviruses had evolved substantially and clustered with viruses seen at the time drugs were started and at rebound, consistent with renewed rounds of replication that expand and diversify the reservoir. Together with the low levels of viral RNA in controllers, these findings support a “block‑and‑lock” situation: the remaining intact proviruses are few and relatively silent, making them less likely to reignite infection even without daily drugs.
What this means for future HIV remission trials
This work shows that durable control of virus after stopping therapy depends on both the size and the behavior of the hidden reservoir and on the strength and quality of the immune response, especially CD8 T cells in lymph nodes. In the macaque model, a small pool of intact proviruses in lymph nodes before treatment interruption—and a stable, low level of intact proviruses in blood shortly afterward—signal a good chance of long‑term control. While these findings need to be translated and tested in people, they point toward practical biomarkers to guide when it may be safer to pause therapy in cure‑oriented studies and emphasize that boosting the right kind of immune response could help turn short‑term viral suppression into lasting drug‑free remission.
Citation: Charre, C., Melard, A., Chaillon, A. et al. Post-treatment SIV control is associated with specific features of viral persistence before and after treatment interruption. Nat Commun 17, 3290 (2026). https://doi.org/10.1038/s41467-026-69720-6
Keywords: HIV remission, viral reservoir, CD8 T cells, treatment interruption, nonhuman primate model