Clear Sky Science · en
Roles of the peroxisome proliferator-activated receptors (PPARs) in the pathogenesis of diabetic kidney disease (DKD)
Why this kidney story matters
Diabetic kidney disease is one of the most serious long term complications of diabetes and a leading reason people need dialysis or a kidney transplant. This review article explores a family of molecular switches inside kidney cells that help control how those cells use energy, handle fats and sugars, and respond to irritation and scarring. Understanding how these switches work, and how they differ from one kidney cell type to another, could open the door to more precise treatments that slow or even halt kidney damage in people with diabetes.
Key players in diabetic kidney damage
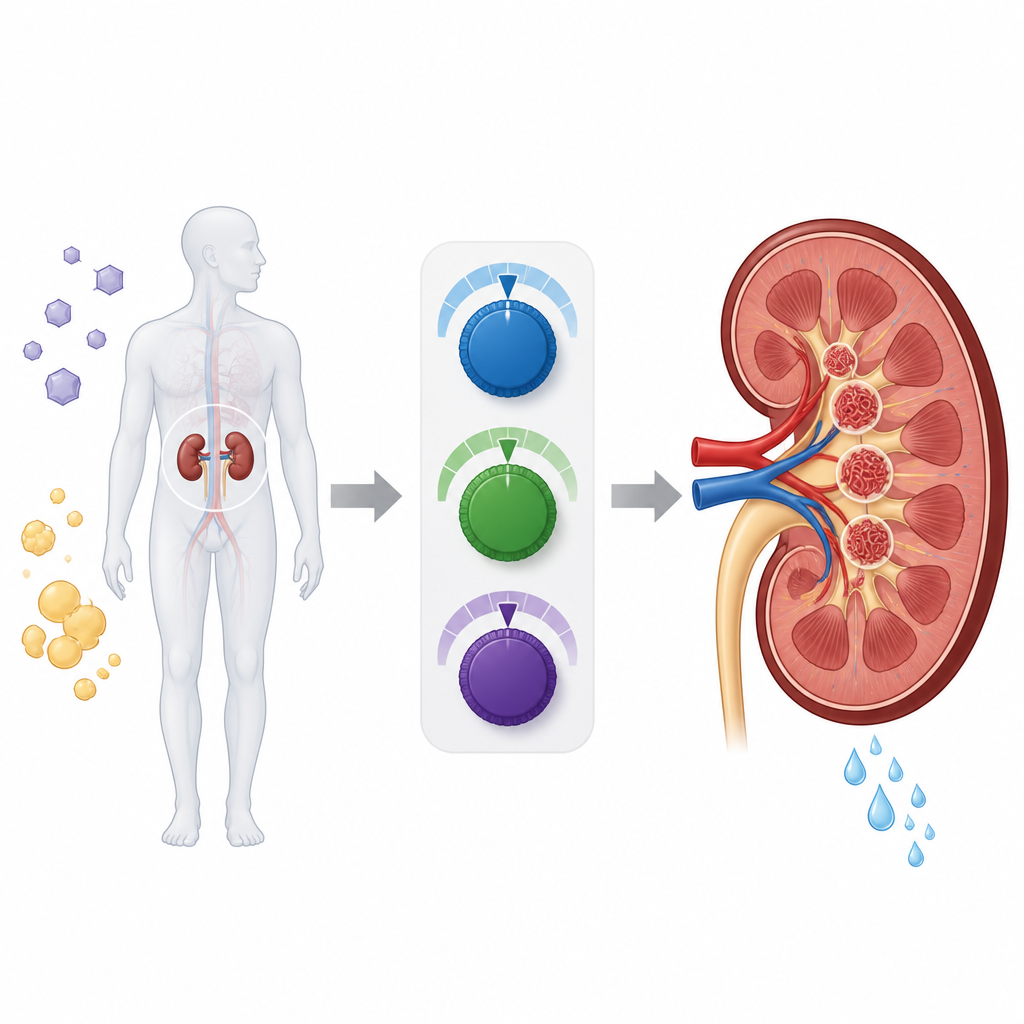
Diabetic kidney disease develops slowly as high blood sugar, altered blood flow, and toxic sugar fat byproducts strain the kidney’s filters and tubules. Over time, this strain leads to leakage of protein into the urine, loss of filtering units, and scarring of the supporting tissue. The paper focuses on three related proteins called PPARs that sit in the cell nucleus and influence which genes are turned on. Each subtype, known as alpha, gamma, and beta/delta, has its own pattern of activity in the kidney. Together, they help manage fuel use, fat breakdown, inflammation, and scar formation. When their activity becomes unbalanced in diabetes, harmful cycles of fat overload, oxidative stress, and fibrosis are reinforced.
Different switches in different kidney cells
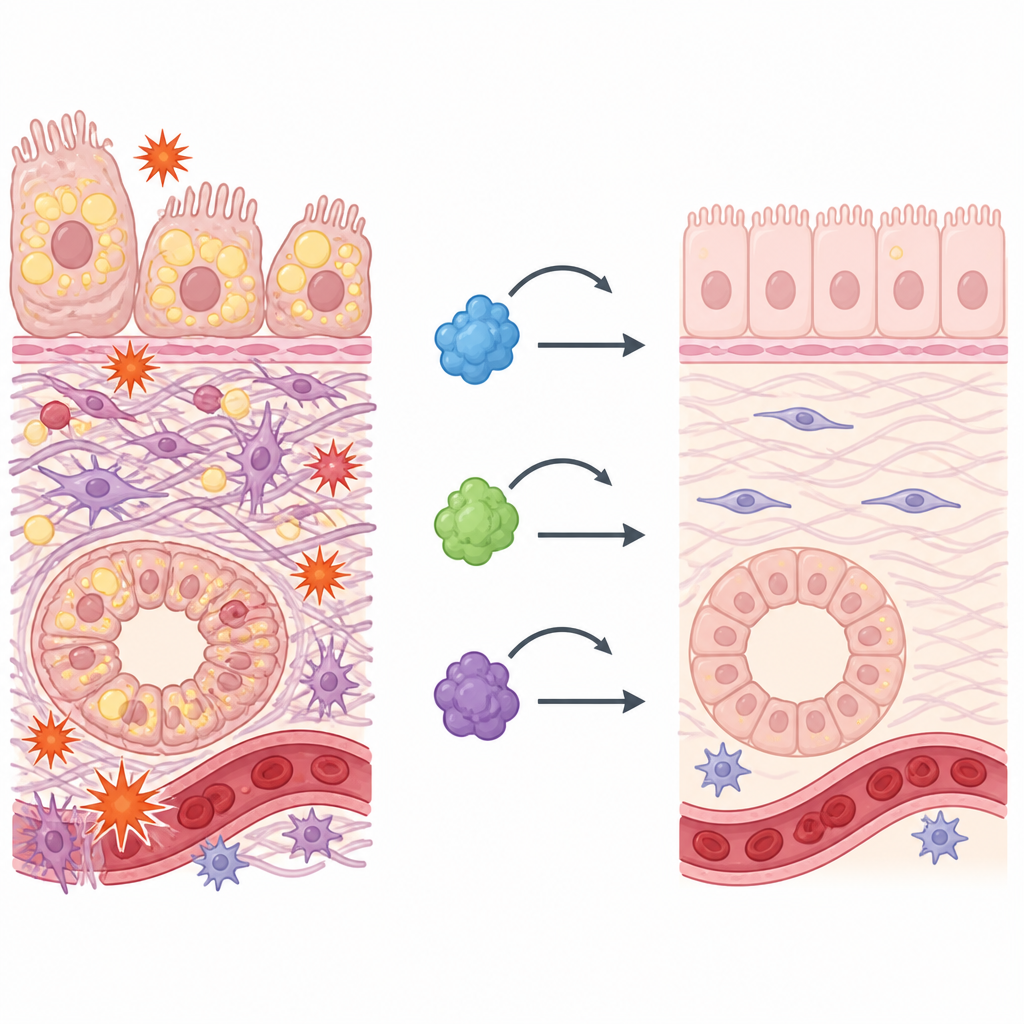
The authors adopt a cell by cell view of the kidney. In podocytes, the delicate cells that wrap around the filtering capillaries, PPAR gamma and PPAR alpha help maintain cell survival by supporting self cleaning (autophagy), defending against oxidative stress, and promoting healthy fat burning. When these switches are blocked or misdirected by other molecules, podocytes lose their special structure, die, or transform into more fibrotic cell types, weakening the filter. In mesangial cells, which sit in the center of the filter unit, PPAR gamma acts as a brake on inflammatory signals and overproduction of collagen and other matrix proteins that thicken and stiffen the filter. PPAR alpha and PPAR delta work alongside it to improve fat handling and limit toxic signals triggered by sugar modified proteins.
Guardians of the kidney tubes and blood vessels
Further along the nephron, in the tubular cells that reabsorb salts, water, and nutrients, PPAR alpha and PPAR gamma again take center stage. Here, PPAR alpha boosts burning of fatty acids and supports healthy communication between mitochondria and other cell structures, preventing fat droplets from piling up and injuring the cells. PPAR gamma helps curb inflammatory pathways and slows the process by which tubular cells adopt scar like features, a step that drives interstitial fibrosis. In the lining cells of kidney blood vessels, PPAR alpha activity improves vessel function, reduces recruitment of aggressive immune cells, and works with the hormone adiponectin to counteract the effects of chronic high sugar.
Breaking the cycle of fat, fire, and scar tissue
Across these cell types, the review highlights a common thread: diabetic kidney disease is maintained by a self reinforcing loop of disturbed metabolism, chronic inflammation, and scar formation. PPAR signaling sits at the center of this loop. When PPAR alpha driven fat burning falters, mitochondria generate more reactive molecules that further inflame tissue. When PPAR gamma and related pathways are suppressed, protective signals such as adiponectin and anti fibrotic genes weaken, allowing scarring to spread. The authors also discuss how genetic differences in PPAR genes can alter an individual’s susceptibility to kidney damage, although the impact varies between populations and between type 1 and type 2 diabetes.
New treatment ideas from a cell focused view
Clinically, drugs that act on PPARs already exist, such as fenofibrate and the thiazolidinedione class, and some studies suggest they can reduce protein loss in urine and slow kidney function decline. However, side effects like fluid retention and heart problems limit their use, and present medicines do not target specific kidney cell types. This review proposes future strategies that include combining multiple PPAR targets, designing “pan PPAR” drugs that balance all three subtypes more safely, and using nanotechnology or tiny vesicles to deliver therapies directly to podocytes, tubules, or blood vessel cells. By tailoring treatments to the unique PPAR roles in each kidney cell, the hope is to interrupt the damaging cycle of metabolic stress, inflammation, and fibrosis more effectively and with fewer unwanted effects.
Citation: Zheng, Z., Li, Y. & Pan, Y. Roles of the peroxisome proliferator-activated receptors (PPARs) in the pathogenesis of diabetic kidney disease (DKD). Cell Death Discov. 12, 219 (2026). https://doi.org/10.1038/s41420-026-03117-8
Keywords: diabetic kidney disease, PPAR signaling, renal fibrosis, lipotoxicity, nanotechnology therapy