Clear Sky Science · en
Incorporating early cfEBV DNA clearance into clinical risk stratification to tailor induction chemotherapy cycles for locoregionally advanced nasopharyngeal carcinoma
Why this study matters to patients and families
For people diagnosed with a cancer behind the nose called nasopharyngeal carcinoma, doctors often give several rounds of chemotherapy before radiation. But more is not always better. This large study explores a simple blood test that tracks traces of a virus linked to the cancer and uses it to decide who truly needs an extra round of chemotherapy and who does not. The goal is to keep the benefits of strong treatment while avoiding needless side effects and delays.
A cancer closely tied to a common virus
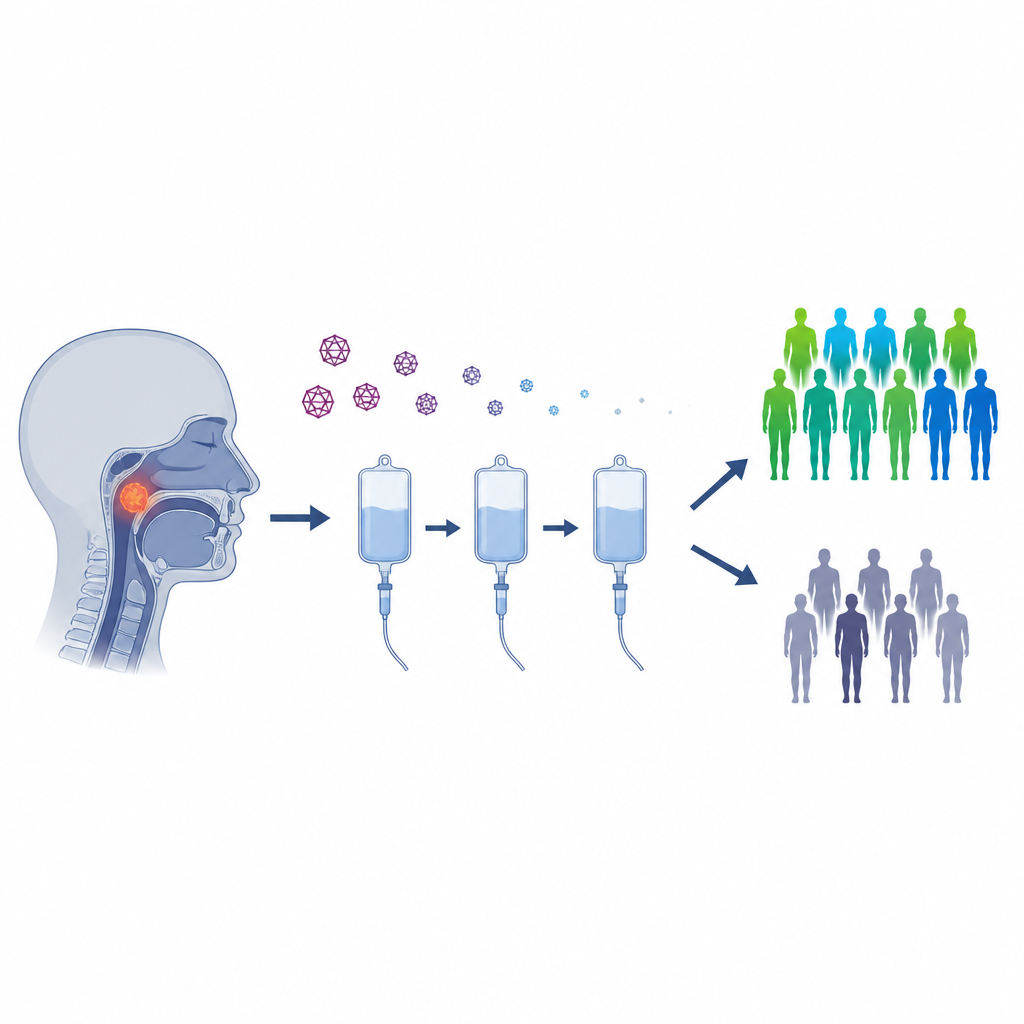
Nasopharyngeal carcinoma is much more common in parts of East and Southeast Asia. Many of these tumors are driven by Epstein-Barr virus, the same virus that can cause “mono.” Tumor cells can release tiny fragments of the virus’s genetic material into the bloodstream, known as cell-free EBV DNA. Measuring these pieces in a blood sample offers a way to estimate how much cancer is present without a scan or biopsy. Because blood tests are quick and repeatable, they are attractive tools for guiding treatment in real time.
Using a blood signal to sort risk early
The researchers examined 1590 patients with locally advanced nasopharyngeal cancer treated at a single major center between 2013 and 2023. All received two or three cycles of chemotherapy before radiation plus chemotherapy. Everyone had blood drawn before treatment and again after the first cycle to measure EBV DNA. After just one cycle, about 45% of patients already had no detectable viral DNA. The team found that three pieces of information together gave the clearest picture of future risk: how far lymph nodes were involved in the neck, the overall clinical stage, and whether EBV DNA had disappeared after the first cycle.
Dividing patients into lower and higher risk paths
Using those three factors, the researchers built a score and split patients into low-risk and high-risk groups. People in the low-risk group had better survival overall, while those in the high-risk group were more likely to see the cancer return or spread. This simple scoring system performed better than traditional staging or the blood test alone when predicting whether patients would be free of disease five years later. In other words, the early change in EBV DNA acted like a quick “report card” on how well the cancer was responding to the first hit of chemotherapy.
Who benefits from an extra chemotherapy cycle
The key question was whether everyone should receive three cycles of induction chemotherapy, or whether some could stop after two. To make a fair comparison, the team carefully matched patients with similar ages, disease features, and treatments aside from the number of cycles. In the low-risk group, those who received three cycles had clearly better chances of remaining free of progression and of living longer, with similar rates of serious side effects compared with two cycles. In contrast, in the high-risk group, adding a third cycle did not improve any major survival measure. For these patients, a longer course of early chemotherapy mainly brought extra nutritional strain and more low blood protein, without clear benefit.

What this means for future care
This study suggests that a simple early blood test, combined with standard staging, can help tailor how much chemotherapy a person with nasopharyngeal cancer really needs before starting radiation. Patients whose viral DNA vanishes quickly and whose disease is not at the most advanced local stage may gain from an extra cycle, likely by better clearing hidden cancer cells elsewhere in the body. Those who remain high risk after the first cycle may be better served by moving sooner to radiation or exploring other options such as immunotherapy instead of piling on more of the same chemotherapy. While the results need to be confirmed in other hospitals and populations, they point toward a future in which treatment for this virus-linked cancer is not one-size-fits-all, but guided by how each patient’s tumor responds in real time.
Citation: Guo, WP., Yu, X., Lu, ZJ. et al. Incorporating early cfEBV DNA clearance into clinical risk stratification to tailor induction chemotherapy cycles for locoregionally advanced nasopharyngeal carcinoma. Br J Cancer 134, 1557–1567 (2026). https://doi.org/10.1038/s41416-026-03401-5
Keywords: nasopharyngeal carcinoma, Epstein Barr virus, liquid biopsy, induction chemotherapy, risk stratification