Clear Sky Science · en
Effectiveness of linvoseltamab versus real-world standard-of-care in triple-class-exposed relapsed/refractory multiple myeloma in the United States
New hope for people with tough-to-treat myeloma
For people living with multiple myeloma whose cancer has already pushed past several modern drug types, treatment choices often become a maze of complex drug cocktails with modest benefit. This study looks at whether a newer targeted antibody drug, linvoseltamab, can give these heavily treated patients better and longer-lasting control of their disease than the varied treatments doctors currently use in everyday practice across the United States.
When standard drug groups stop working
Multiple myeloma is a cancer of plasma cells in the bone marrow. Many patients today receive powerful combinations of three or four drugs, including proteasome inhibitors, immunomodulatory pills, and antibodies that target a marker called CD38. Over time, however, many patients become exposed to, or even resistant to, all three major drug classes. At that point, options shrink, and survival is typically limited. Although advanced treatments such as CAR T cell therapy and other bispecific antibodies exist, they have been slow to reach many patients, especially those treated in community clinics rather than large academic centers.
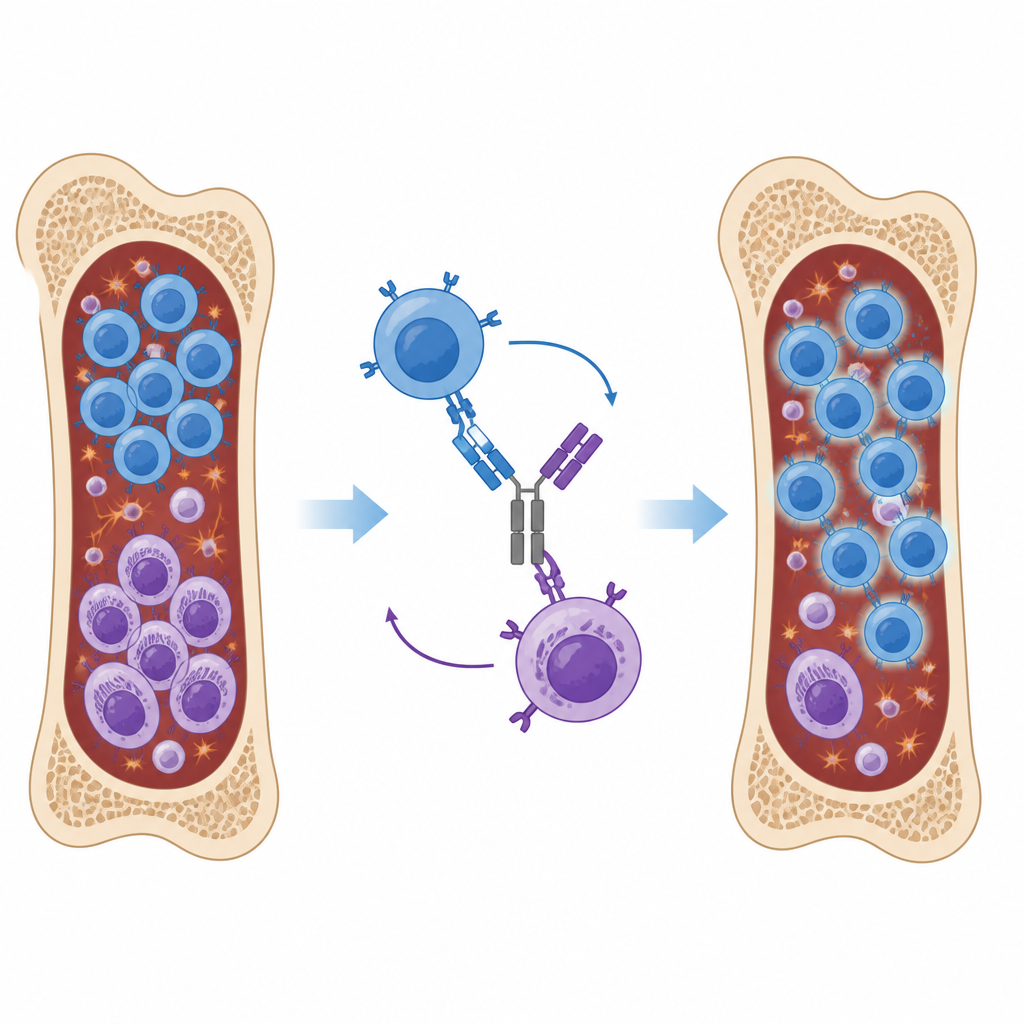
A new antibody that links immune cells to cancer cells
Linvoseltamab is a lab-made antibody designed to latch onto two different targets at once: BCMA on myeloma cells and CD3 on T cells, a key part of the immune system. By physically bringing T cells and myeloma cells together, it encourages the immune system to attack and kill the cancer cells. Earlier clinical trials of linvoseltamab showed deep and durable responses in patients whose disease had already resisted multiple treatments, but it had not yet been compared against the many regimens doctors actually choose in routine care.
Comparing trial patients with real-world care
The researchers compared 105 patients receiving linvoseltamab in a phase 2 clinical trial with 149 similar patients treated at US centers whose information was stored in electronic health records. All had advanced myeloma that had been treated with at least three prior lines of therapy and were exposed to the three main drug classes. Real-world patients received 87 different treatment combinations, most commonly mixes of carfilzomib or daratumumab with pomalidomide and dexamethasone. Almost none received CAR T cells or other bispecific antibodies, reflecting the limited use of these newer options in community settings during the study period.
Stronger responses and longer time before disease worsens
Linvoseltamab outperformed real-world standard care across every main measure. About seven in ten linvoseltamab patients saw their cancer shrink noticeably, compared with a little over one in three among those on usual treatments. Deep responses, where cancer levels fell to very low or undetectable levels, were much more common with linvoseltamab. Patients on linvoseltamab also went longer before their disease got worse, needed another treatment, or led to death. Median progression-free survival and time to next treatment had not yet been reached for linvoseltamab at the time of the analysis, while real-world patients saw their disease move again within a few months. Overall survival was longer as well: a median of about 28 months with linvoseltamab versus 10 months with standard care.
Testing the results from many angles
Because the comparison was not a randomized trial, the team used several methods to make the groups as similar as possible. They matched patients on important features such as age, disease risk markers, performance status, and how many prior treatments they had received. An independent committee of myeloma experts and methodologists reviewed the data sources and methods without seeing the outcomes and agreed that the comparison was reasonable. The researchers also ran multiple sensitivity analyses, changing technical definitions of response and survival, and excluding patients with very short predicted life expectancy. In each case, linvoseltamab maintained a clear advantage over real-world care.
What this means for patients and doctors
For people with multiple myeloma whose cancer has already resisted several major drug classes, this study suggests that linvoseltamab can provide higher response rates and longer-lasting control than the mix of treatments many patients currently receive, particularly in community clinics. While these findings come from a careful comparison rather than a head-to-head randomized trial, they indicate that this bispecific antibody may become an important option when standard combinations are no longer working. As access to such therapies expands, more patients with advanced myeloma may be able to live longer and with better disease control.
Citation: Kumar, S., Weisel, K.C., Spin, P. et al. Effectiveness of linvoseltamab versus real-world standard-of-care in triple-class-exposed relapsed/refractory multiple myeloma in the United States. Blood Cancer J. 16, 72 (2026). https://doi.org/10.1038/s41408-026-01470-6
Keywords: multiple myeloma, linvoseltamab, bispecific antibody, relapsed refractory cancer, real-world evidence