Clear Sky Science · en
Network meta-analysis to compare the efficacies of three surgical techniques in rheumatic mitral valve disease
Why fixing a heart valve is not one-size-fits-all
For millions of people worldwide, especially in low- and middle-income countries, a childhood strep infection can silently scar the heart and narrow a key valve, the mitral valve. When this valve becomes too tight, the heart struggles to pump blood, causing breathlessness, fatigue, and eventually heart failure. Today, doctors can open or replace the valve using several techniques, but there is ongoing debate over which option gives patients the best balance of safety and long-term benefit. This study brings together evidence from more than 15,000 patients to compare three main procedures head‑to‑head.
Three different ways to tackle a tight valve
The paper focuses on rheumatic mitral valve disease, damage caused by long‑standing inflammation after rheumatic fever. The authors compare three treatments. The first, percutaneous mitral balloon commissurotomy (PMBC), is a catheter‑based “balloon” procedure done through a blood vessel without opening the chest. The second, mitral valvuloplasty (MVP), is an open‑heart operation in which surgeons repair the patient’s own valve, reshaping and supporting it so it works better. The third, mitral valve replacement (MVR), removes the damaged valve and swaps it for an artificial one, either mechanical (which requires lifelong blood thinners) or biological (which can wear out over time). Current guidelines typically place PMBC first in line, using surgery only when the catheter procedure is not suitable.
Pulling together evidence from around the world
To look beyond one‑to‑one comparisons, the researchers performed a network meta‑analysis, a statistical approach that can compare several treatments at once using both direct and indirect evidence. They sifted through nearly 10,000 scientific reports and ultimately included 23 studies—both randomized trials and observational cohorts—covering 15,271 adults with rheumatic mitral valve disease. Of these, 894 patients had PMBC, 2,972 had MVP, and 11,405 had MVR. The team examined early deaths within 30 days of the procedure, deaths and complications during follow‑up, and how often patients needed another valve procedure later on.
Short‑term safety versus long‑term durability
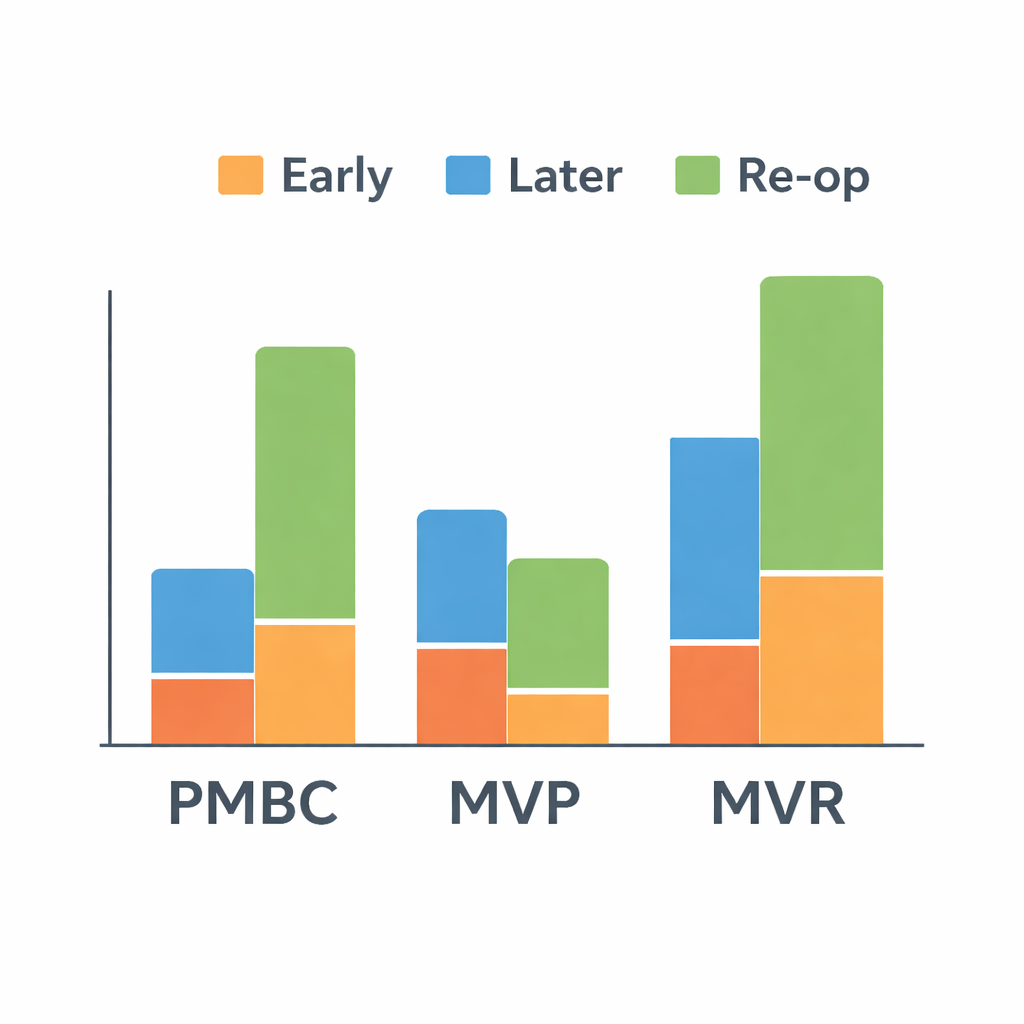
The analysis found clear trade‑offs. PMBC, the balloon procedure, had the lowest risk of dying soon after treatment, likely because it avoids major surgery. Both PMBC and MVP had better early survival than valve replacement. Over the longer term, however, repairing the valve (MVP) seemed to offer the best balance: patients who had MVP were less likely to die or suffer major complications such as blood clots, bleeding, or severe valve problems than those who received an artificial valve. At the same time, they needed fewer repeat procedures than patients treated with PMBC, which is known to have a higher chance of the valve narrowing again.
Not all repairs are created equal
The study also drilled deeper into how repair is done. Some surgeons performed only a simple cut to loosen the stiff parts of the valve (simple commissurotomy), while others used a more complete “composite” repair that might include sewing a supporting ring, trimming thickened tissue, and freeing the valve’s supporting structures. Patients who received this more thorough composite repair had better survival and fewer complications than those whose valves were merely loosened, and they still accepted a somewhat higher chance of later reoperation compared with full replacement. In other words, the quality and extent of the repair mattered greatly for patient outcomes.
What this means for patients and doctors
For people living with rheumatic mitral valve disease, the message of this study is that keeping and carefully rebuilding the natural valve often leads to better long‑term health than replacing it outright, provided the valve is suitable for a comprehensive repair. Balloon procedures remain valuable, especially for patients who cannot safely undergo surgery, but they may increase the chance that more invasive surgery is needed later. The authors suggest that, when anatomy and surgical expertise allow, advanced valve repair should be the preferred option, with replacement reserved for cases where repair is not feasible. Ultimately, they argue that treatment should be tailored to each patient, ideally using modern imaging tools to predict who is most likely to benefit from repair, and they call for new clinical trials to confirm and refine these recommendations.
Citation: Liu, C., Jia, Sh., Wang, Mz. et al. Network meta-analysis to compare the efficacies of three surgical techniques in rheumatic mitral valve disease. npj Cardiovasc Health 3, 6 (2026). https://doi.org/10.1038/s44325-026-00106-9
Keywords: rheumatic heart disease, mitral valve repair, balloon valvotomy, valve replacement, heart surgery outcomes