Clear Sky Science · en
A narrative review of impacts of apolipoproteins on atherosclerotic coronary plaques
Why the Fats in Your Blood Still Matter
Heart attacks and strokes often begin with silent changes in the blood vessels that feed the heart. This article looks beyond familiar "good" and "bad" cholesterol to the protein shells that carry fats through the bloodstream, called apolipoproteins. By following how four of these proteins shape the growth, make-up, and treatment of coronary plaques – the fatty buildups that clog heart arteries – the authors show why some people remain at high risk for heart disease even when their cholesterol numbers look ideal.
The Hidden Players Riding on Cholesterol
Most of us hear about LDL and HDL cholesterol, but each of these particles is wrapped in one or more apolipoproteins that help decide where the particle goes and how dangerous it is. This review focuses on four key types: apolipoprotein(a), apolipoprotein A‑I, apolipoprotein B, and apolipoprotein C‑III. Together they govern how fatty particles are assembled, how long they stay in circulation, and how easily they enter and damage the artery wall. Modern imaging tools – ultrasound inside the artery, high‑resolution light-based scans, and CT angiography – now allow doctors to see not just how narrow an artery is, but whether its plaques are soft and rupture‑prone or dense and calcified. 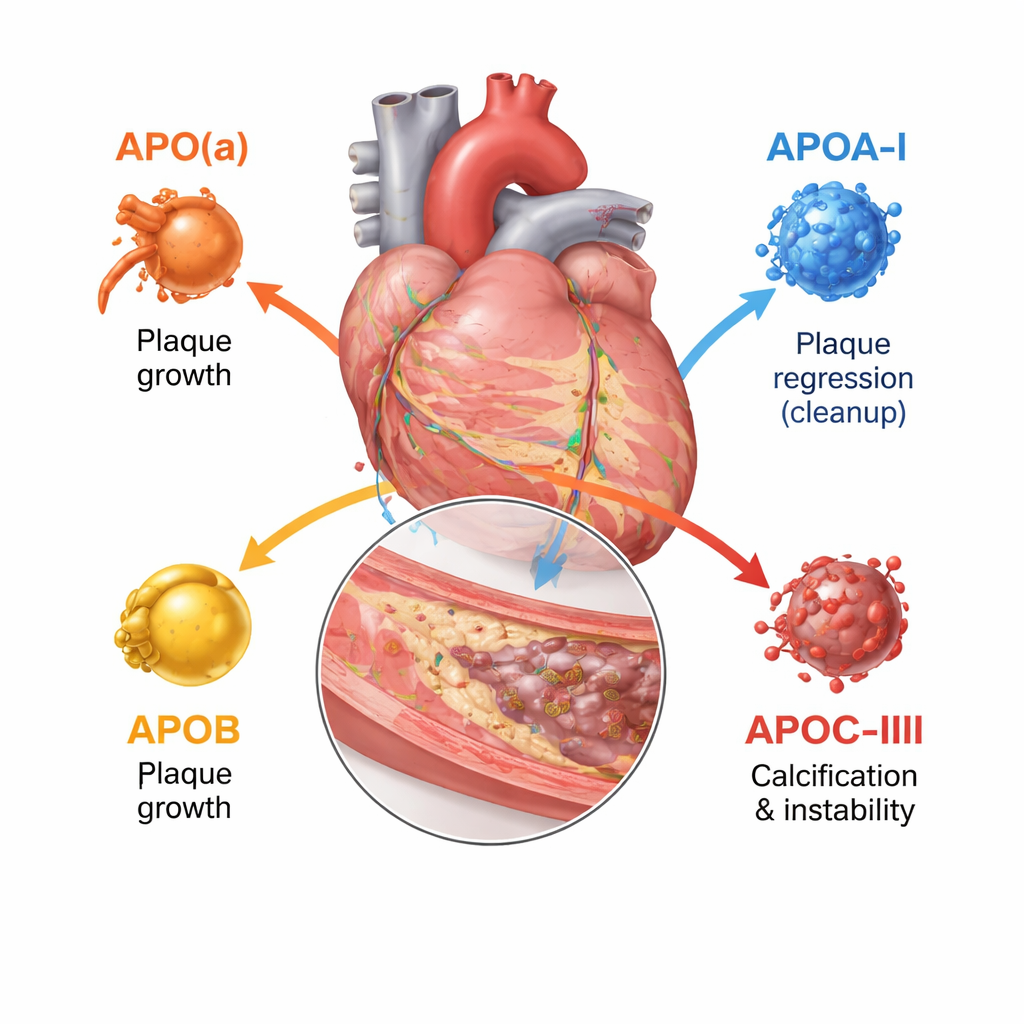
How Four Proteins Shape Dangerous Plaques
Apolipoprotein B sits on every LDL and similar particle and effectively counts how many atherogenic – artery‑clogging – particles are in the blood. The more ApoB‑bearing particles a person has and the longer they circulate, the greater the total plaque burden in coronary arteries. Studies using imaging inside heart arteries show that higher ApoB levels go hand in hand with larger plaques, longer lesion length, more soft, necrotic cores, and fewer stabilizing calcium deposits. In contrast, apolipoprotein A‑I, the main protein on HDL, helps remove cholesterol from plaque cells and carry it back to the liver. Higher functional ApoA‑I activity and a favorable balance of HDL cholesterol to ApoA‑I are linked with slower plaque growth and more fibrous, stable tissue, although simply raising HDL cholesterol in the bloodstream has not translated into fewer events.
A Special Risk Protein and a Promoter of Hardening
Apolipoprotein(a) forms a particle called lipoprotein(a), or Lp(a), when it attaches to an LDL-like core. Lp(a) is almost entirely determined by genetics and usually unaffected by diet. Imaging studies in thousands of patients show that people with high Lp(a) have more overall plaque, more low‑density, lipid‑rich regions, and more focal “high‑risk” plaques that are prone to rupture, even when LDL cholesterol is already treated aggressively. The review concludes that Lp(a) represents a major “residual risk” that standard cholesterol‑lowering therapies do not fully address. Apolipoprotein C‑III, mostly found on triglyceride‑rich particles, slows their clearance and stirs inflammation. People with higher ApoC‑III have more coronary calcium and more complex, calcified nodules inside plaques, features tied to advanced disease and stiffening of the arteries.
New Medicines Aiming at the Right Targets
Because these proteins track risk more precisely than cholesterol alone, they are becoming direct drug targets. For Lp(a), several injectable genetic medicines – antisense and small‑interfering RNA drugs – can cut levels by 80–95% in early trials, and a pill that blocks assembly of the particle also shows large reductions. For ApoC‑III, recently approved therapies can sharply lower triglycerides and ApoC‑III itself, and early data suggest they may reduce pancreatitis and could reshape plaque calcification. 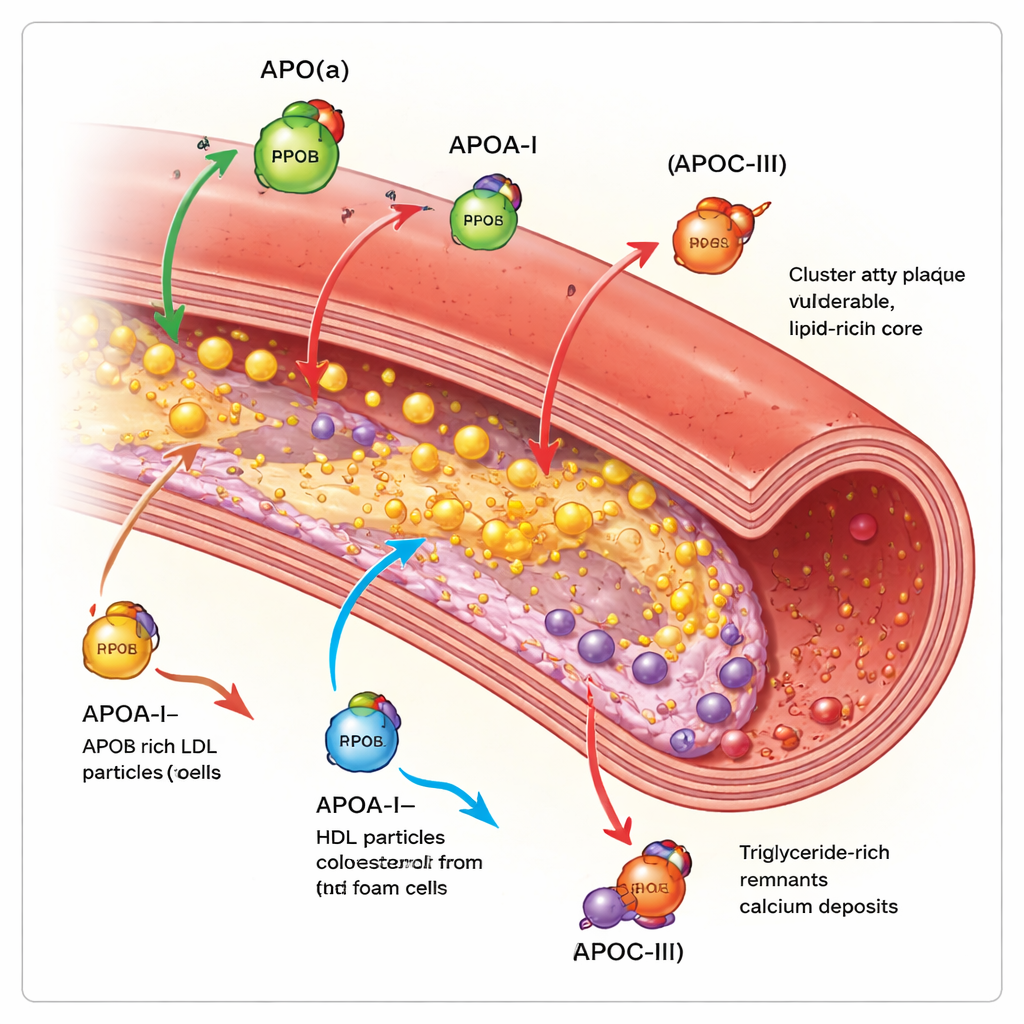
What This Means for Protecting Your Heart
In simple terms, this review argues that who gets a heart attack is not decided by cholesterol levels alone, but by the mix and behavior of the protein‑coated particles carrying that cholesterol. ApoB reflects how many “bad” particles bombard the artery wall, ApoA‑I reflects the system that hauls cholesterol away, Lp(a) adds an extra, genetically set risk, and ApoC‑III favors hardened, inflamed plaques. Emerging drugs that specifically dial down Lp(a) and ApoC‑III, and more precise use of ApoB and ApoA‑I in routine testing, could allow doctors to tailor prevention to the individual plaque biology of each patient, catching hidden risk that standard lipid panels miss.
Citation: Fukase, T., Dohi, T. A narrative review of impacts of apolipoproteins on atherosclerotic coronary plaques. npj Cardiovasc Health 3, 4 (2026). https://doi.org/10.1038/s44325-026-00104-x
Keywords: lipoprotein(a), apolipoprotein B, apolipoprotein A-I, apolipoprotein C-III, coronary plaque imaging