Clear Sky Science · en
Rethinking endometriosis recurrence: from clinical challenge to biological opportunity
Why this matters to everyday life
Endometriosis affects millions of people worldwide, often causing severe pain, fatigue, and fertility problems. Surgery can bring real relief, but for many, the symptoms or lesions come back. This review looks at why endometriosis so often returns after an operation, and how that “recurrence” may actually be a window into the biology of the disease—and a chance to develop more personal, longer-lasting treatments.
When “coming back” can mean different things
Doctors and researchers do not yet agree on a single definition of endometriosis recurrence. Sometimes it means that pain returns after a period of relief; other times it means that new or larger lesions are seen on scans or during another surgery. These two events often overlap but not always. Some people have painful symptoms even when no clear lesions are visible, while others show lesion regrowth but feel fine. Pain can stem from changes in the nervous system, scarring, or other pelvic conditions, not just from the size or number of lesions. This mismatch makes it hard to compare studies and to give patients clear expectations about what surgery can and cannot achieve.
How doctors currently track and try to prevent return
Because repeat surgery is invasive and can damage the ovaries, most follow-up relies on ultrasound or MRI, which are good at spotting large ovarian cysts but may miss small or hidden lesions elsewhere. There is no simple blood test that reliably tracks endometriosis activity over time. Researchers have started to build prediction tools using clinical factors—such as age, the extent of disease at surgery, and the presence of adhesions—as well as experimental tissue and blood markers. Younger age, more severe disease, large cysts, and strong preoperative pain tend to increase the chance of recurrence, while pregnancy and long-term hormonal suppression tend to reduce it. Yet current prediction models are modest and need testing in larger, more diverse groups of patients.
Hormones help, but rarely cure
Long-term hormonal treatment after surgery—for example, continuous birth control pills or hormone-releasing devices in the uterus—can cut the risk of lesions and pain returning by roughly one-third to two-thirds. These medicines work mainly by keeping estrogen levels low and menstrual cycling quiet, which starves endometriosis tissue and calms inflammation. However, their protection fades quickly once treatment stops, and side effects, personal preference, or the desire for pregnancy often limit how long they can be used. Some patients also seem biologically “resistant” to certain hormones, especially progestins, or have pain driven by nerve and brain changes that hormones do not fully address. As a result, many people still face a cycle of symptom flare, treatment, and relapse.
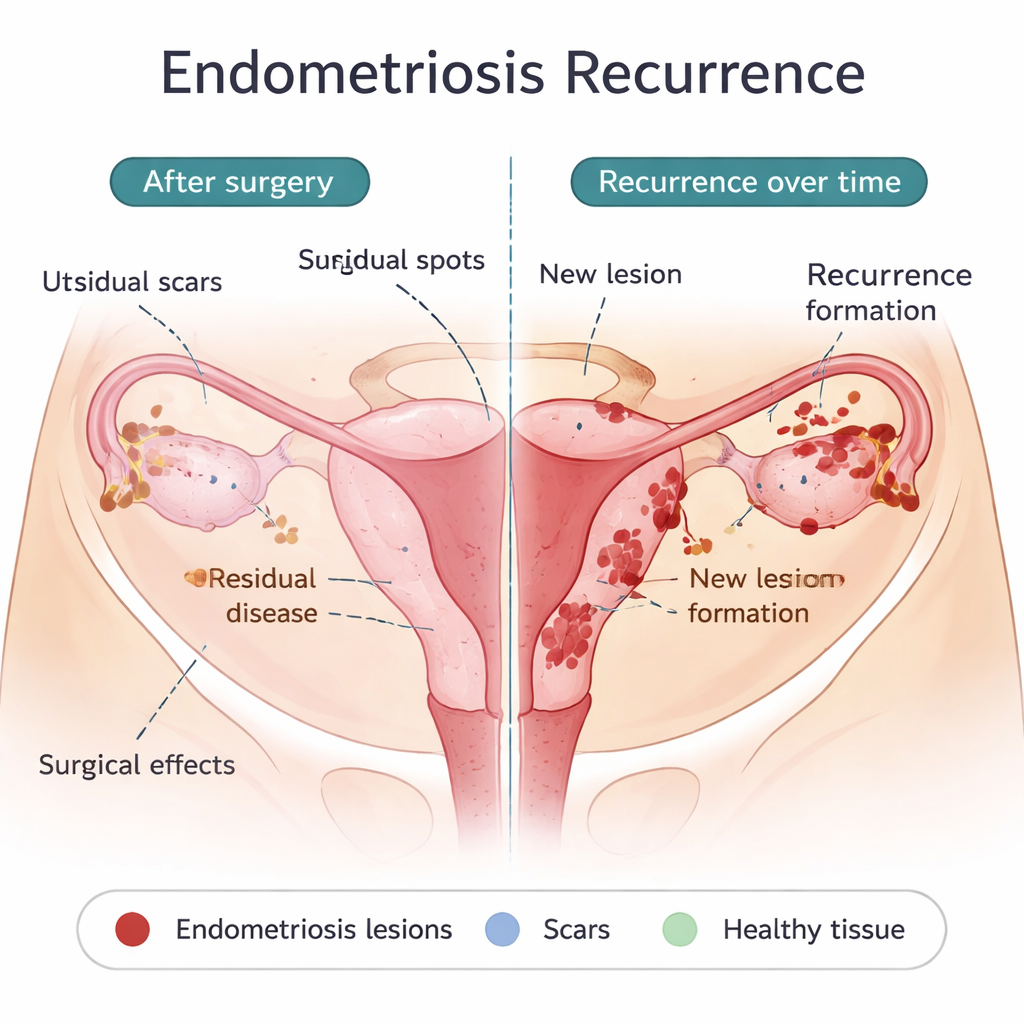
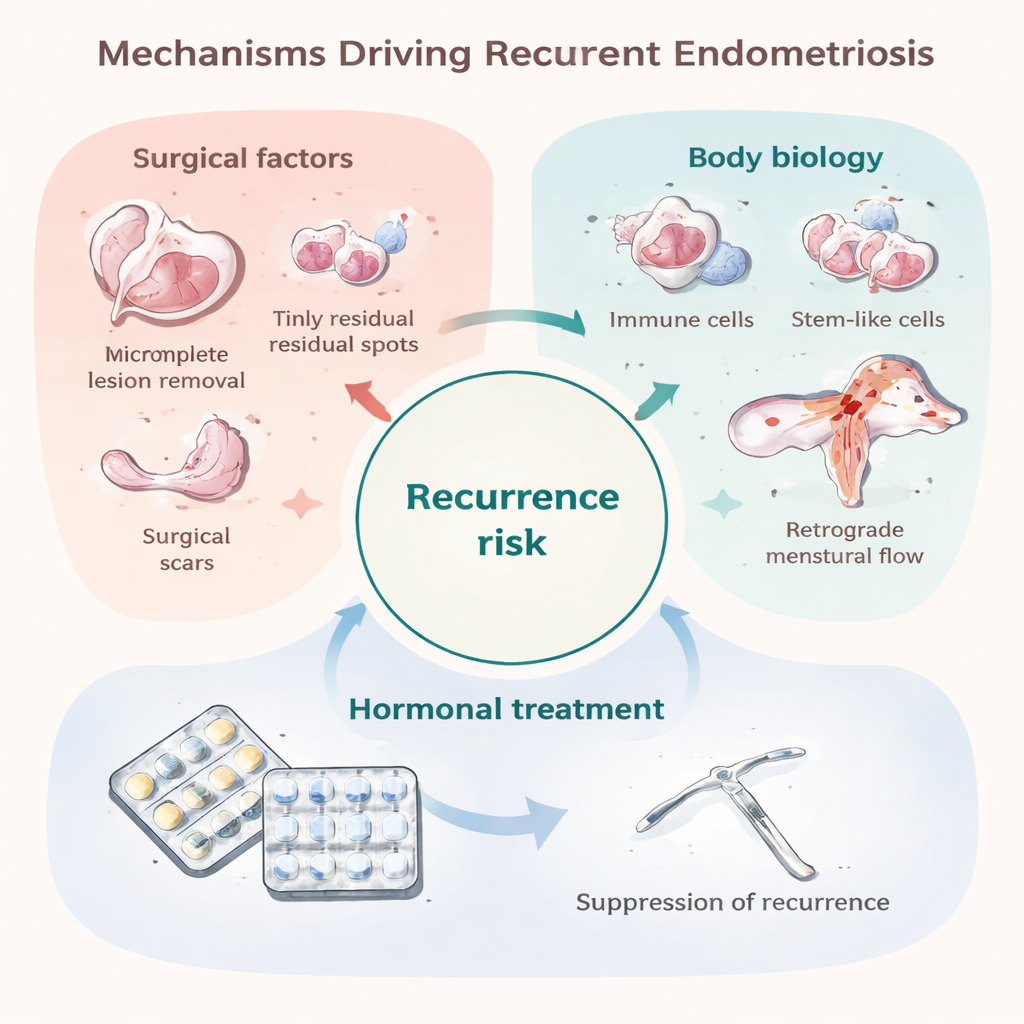
What surgery may leave behind—and what may be truly new
One major reason for early recurrence is minimal residual disease: tiny implants that were not or could not be removed during the first operation. These may be invisible to the naked eye yet able to grow once the protective effect of postoperative hormones wears off. Certain surgical choices, like more conservative removal of ovarian cysts, are linked to higher recurrence rates, while more radical excision can reduce recurrence but carries its own risks. Surgery itself may also spread endometrial cells within the abdomen or create scars that offer “fertile soil” for new lesions to take hold. At the same time, some recurrences appear years later or in new locations, suggesting that in at least some patients, new lesions are forming rather than old ones simply regrowing. The same processes thought to cause endometriosis in the first place—menstrual blood flowing backward into the pelvis, an immune system that fails to clear stray cells, stem-like cells that readily implant, and a tolerant, vessel-rich environment—may also drive these later recurrences.
Turning a setback into a biological clue
The authors argue that, instead of seeing recurrence only as surgical failure, it should be treated as a key to understanding endometriosis itself. People whose disease returns despite apparently thorough surgery may have distinctive immune, genetic, or tissue features that make their bodies especially welcoming to endometrial cells. Studying these individuals over time—with standardized ways of measuring symptoms, imaging findings, and lab markers—could reveal which biological pathways truly matter for lesion survival and regrowth. That knowledge could lead to better risk scores, smarter use and duration of hormones, and entirely new treatments that target the roots of the disease rather than just suppressing it. In this way, the frustrating reality of recurrence could become a powerful opportunity to improve long-term, personalized care for those living with endometriosis.
Citation: Masferrer-Ferragutcasas, C., Delgado-Gil, R. & Colas, E. Rethinking endometriosis recurrence: from clinical challenge to biological opportunity. npj Womens Health 4, 4 (2026). https://doi.org/10.1038/s44294-026-00128-9
Keywords: endometriosis recurrence, postoperative hormonal therapy, pelvic pain, personalized gynecology, women’s reproductive health