Clear Sky Science · en
Hierarchical neurocognitive model of externalizing and internalizing comorbidity
Why brains and behavior go hand in hand
Many people live with more than one mental health problem at the same time—for example, a teenager might struggle with both attention difficulties and anxiety. This overlap, called comorbidity, can make diagnosis confusing and treatment less effective. This study followed thousands of young people over a decade and used brain scans and genetics to ask a simple but powerful question: are there common wiring patterns in the brain that help explain why outwardly disruptive problems and inwardly anxious or depressed feelings so often travel together?
Two broad paths of mental struggle
Psychologists often group mental health symptoms into two broad families. One is “externalizing,” which includes acting out, impulsivity, aggression and rule-breaking. The other is “internalizing,” which involves worry, sadness, fear and withdrawal. Instead of focusing on individual diagnoses, the researchers looked across these families of problems in teenagers from a large European study. They had brain scans taken while performing tasks involving stopping an action and anticipating rewards, and they completed detailed questionnaires about their feelings and behavior. By training predictive models, the team asked which patterns of communication between brain regions forecast different symptom types.
Hidden brain patterns behind outward behavior
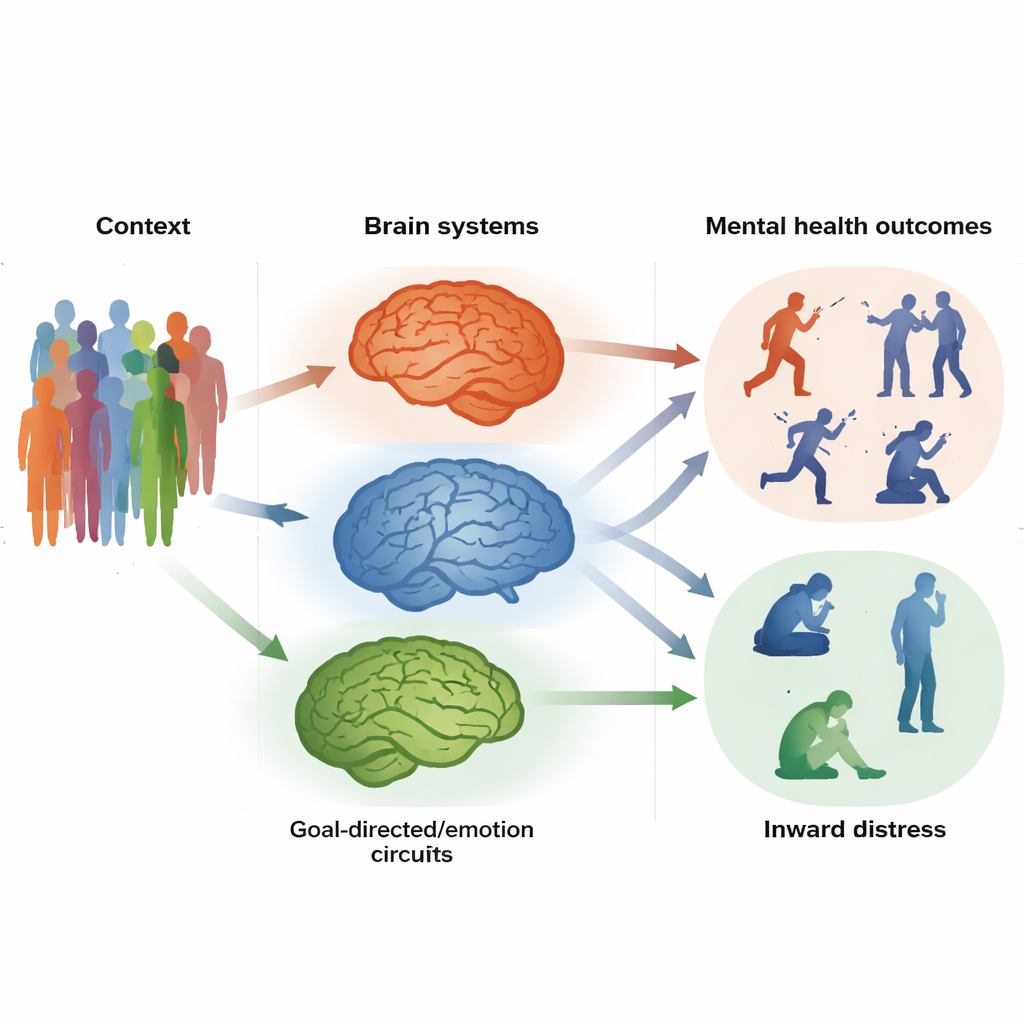
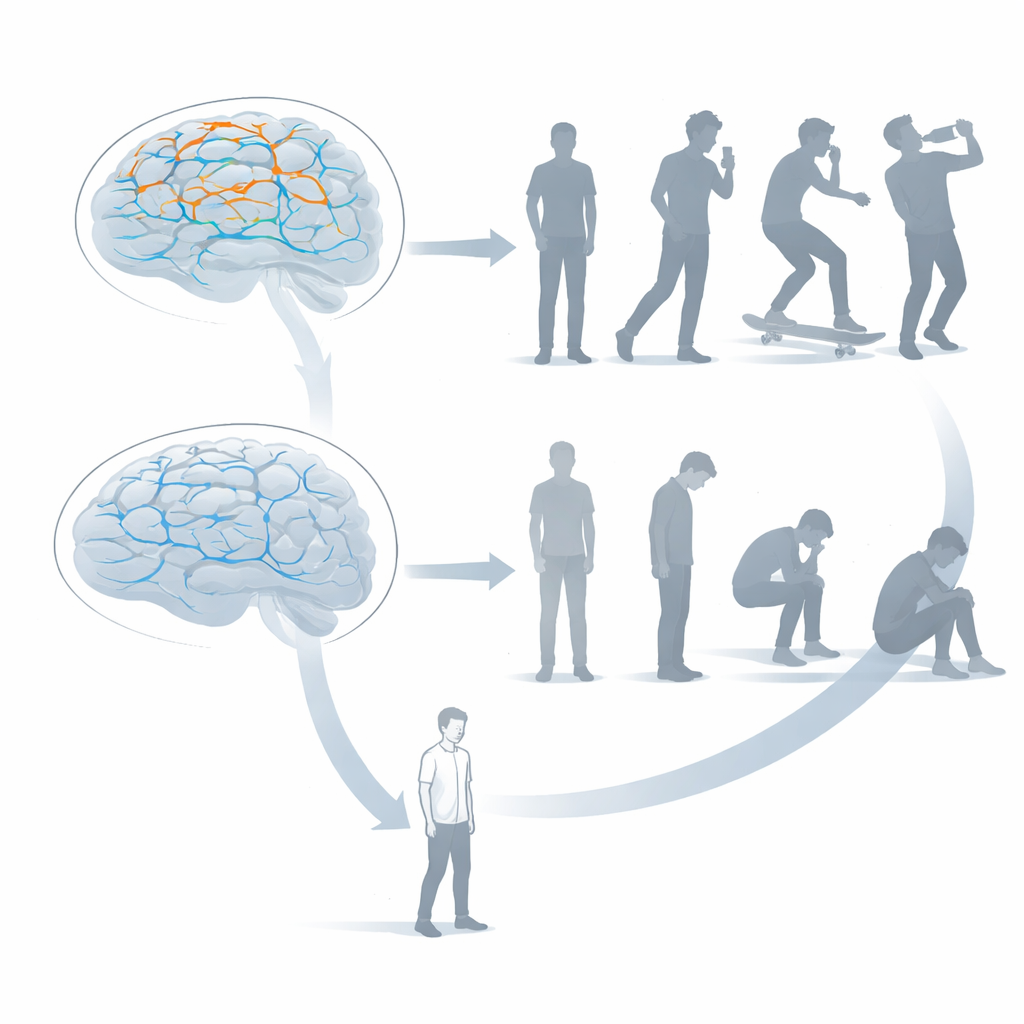
The analyses revealed a distinct “externalizing” brain factor—a set of connections that tended to be stronger in young people with more impulsive and disruptive behaviors. These connections linked areas involved in sensing the outside world and planning movements, including motor regions and a key hub called the middle cingulate cortex. In simple terms, the circuits that prepare the body to act were talking to each other too much. Teenagers with higher scores on this factor not only showed more externalizing symptoms at age 14, but the same pattern of connectivity also predicted similar problems years later and in other groups, including children with attention-deficit/hyperactivity disorder, autism and alcohol use disorder. This suggests that a shared “impulsivity circuit” may underlie many outward-facing difficulties.
Quieted circuits behind inward distress
A second, contrasting “internalizing” brain factor emerged when the team examined symptoms like anxiety, depression, phobias and disordered eating. Here, the telltale pattern was weaker communication among regions in the brain’s decision and valuation centers, including the ventromedial prefrontal and orbitofrontal cortices and the caudate. These regions help us weigh options, learn from feedback and steer our behavior toward long-term goals. When their connections were less active together, teens tended to report more inward distress and personality traits such as high neuroticism and persistent negative thinking. This factor also foreshadowed later internalizing problems and appeared in adults with major depression. In everyday terms, the “goal-setting” and “emotion-guiding” systems seemed underpowered.
One shared control system, two vulnerable circuits
Earlier work from the same group had identified a more general brain factor tied to a wide range of mental health symptoms: an overactive network involved in executive control, the kind of mental traffic cop that should help us focus, plan and hold back unhelpful impulses. Putting the pieces together, the researchers propose a layered model they call NeuroHiP. At the top sits this general inefficiency in control circuits, raising broad vulnerability to mental difficulties. Beneath it lie two more specific layers: an over-wired impulsivity circuit that favors quick, poorly restrained actions, and an under-wired goal-directed circuit that makes it harder to shift out of negative states and pursue helpful behaviors. The balance among these layers may shape whether someone’s struggles show up more on the outside or stay hidden inside.
What this means for prevention and treatment
By mapping outward behavior and inner feelings onto distinct yet overlapping brain systems, this work moves beyond labels like “anxiety” or “ADHD” and toward a more biology-informed picture of mental health. The findings suggest that therapies might be more effective if they are tuned to a person’s underlying neural profile—for example, strengthening goal-directed decision circuits in those prone to rumination, or calming hyperactive motor and reward pathways in those who act before thinking. Because these brain patterns were detectable from preadolescence into adulthood, they may eventually help clinicians identify at-risk youth earlier and offer support tailored not just to their current symptoms, but to the way their brains process control, rewards and emotions over time.
Citation: Xie, C., Xiang, S., Zheng, Y. et al. Hierarchical neurocognitive model of externalizing and internalizing comorbidity. Nat. Mental Health 4, 362–376 (2026). https://doi.org/10.1038/s44220-025-00577-2
Keywords: adolescent mental health, brain connectivity, externalizing disorders, internalizing disorders, psychiatric comorbidity