Clear Sky Science · en
Preoperative lymphocyte signature predicts pancreatic fistula after pancreatoduodenectomy
Why this matters for people facing pancreatic surgery
For people with pancreatic tumors, surgery can be the only real chance of cure—but it is also risky. One of the most serious complications is a leak from the surgical join of the pancreas, called a pancreatic fistula. This problem can keep patients in the hospital longer, cause infections, and delay or even prevent life‑saving chemotherapy. This study asks a simple but powerful question: can a blood test taken before surgery reveal who is most likely to develop this complication, so doctors can prepare and possibly prevent it?
A dangerous leak after a major operation
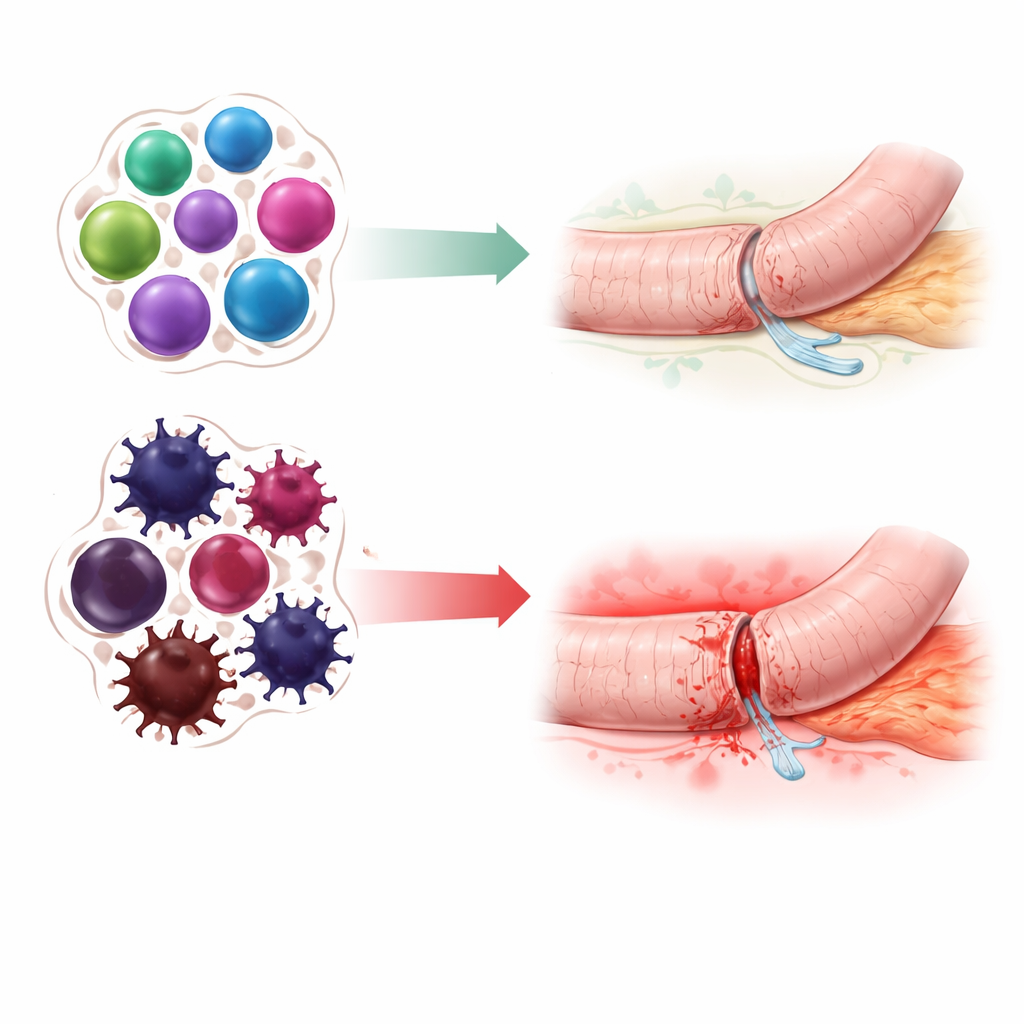
When surgeons remove part of the pancreas in an operation known as pancreatoduodenectomy, they must reconnect the remaining pancreas to the intestines so digestive juices can flow safely. If this new connection leaks, pancreatic enzymes spill into the abdomen and start digesting nearby tissue instead of food. This complication, called postoperative pancreatic fistula, affects roughly one in ten to one in three patients and is a leading cause of serious illness and even death after surgery. It can also derail the entire cancer treatment plan by postponing chemotherapy until the patient recovers—if they recover in time.
Limits of today’s prediction tools
Surgeons already use scoring systems that estimate fistula risk based on factors seen during the operation, like how soft the pancreas feels, how wide the main duct is, and how much blood is lost. While helpful, these scores are partly subjective and only become available once the patient is already in the operating room. Blood tests taken after surgery, such as measures of inflammation or enzyme levels in surgical drains, can flag trouble early but arrive too late to change the initial strategy. The authors argue that what is missing is a clear view of each patient’s biological makeup—especially their immune system—before the first incision is made.
Reading the immune system like a map
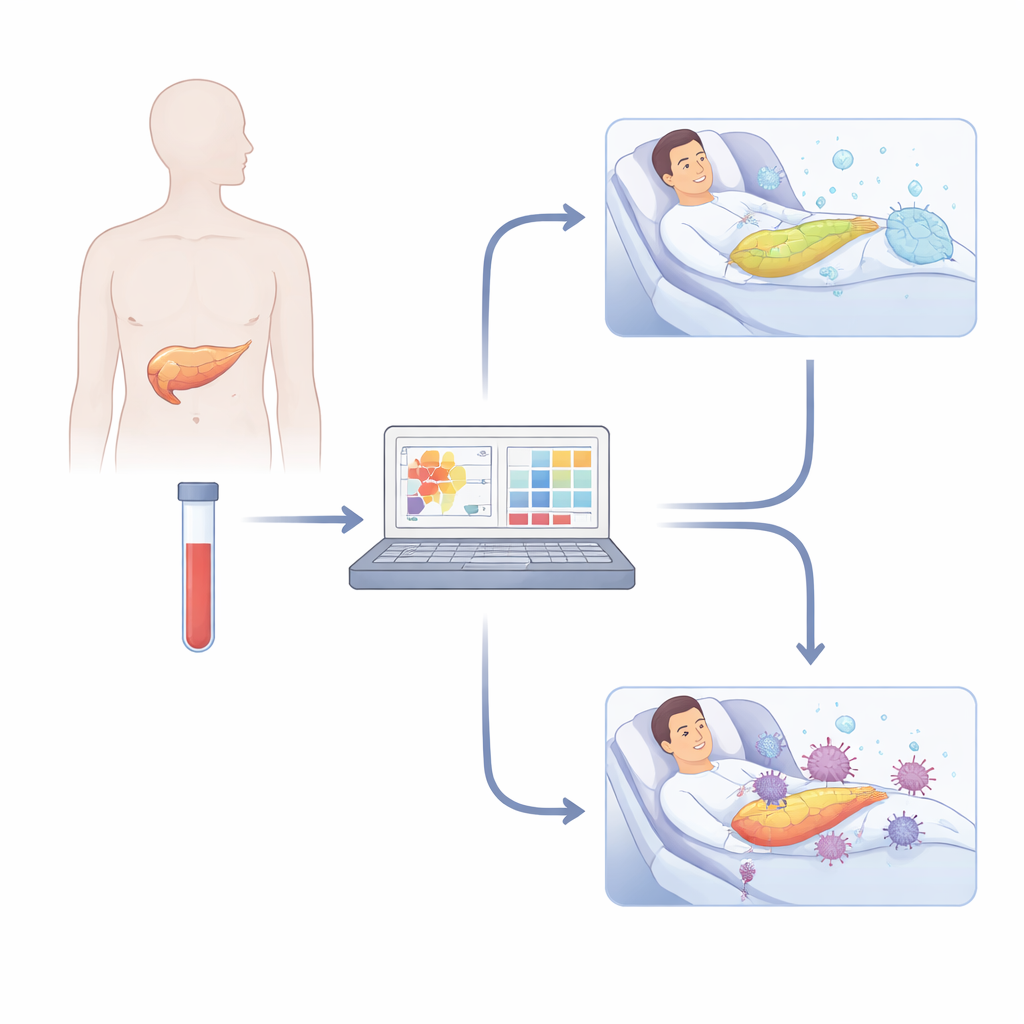
The research team studied 22 patients scheduled for pancreatoduodenectomy as part of the IMMUNOPANC trial. Before surgery, they drew blood and used a cutting‑edge technique called mass cytometry to examine thousands of features on single immune cells at once. They focused on three major types of white blood cells: natural killer cells and two kinds of T cells (CD8 and CD4), which together coordinate how the body responds to injury and infection. Advanced computer methods then grouped these cells into dozens of subtypes based on their surface markers and activity, creating a detailed “map” of each person’s immune landscape. A specialized machine‑learning pipeline, designed to sift through many variables without overfitting, searched this map for combinations of cell types that distinguished patients who later developed a pancreatic fistula from those who did not.
A pre‑surgery “signature” of higher risk
Eight of the 22 patients went on to develop a clinically important pancreatic fistula. The algorithm identified an 11‑part immune signature—mostly involving specific flavors of natural killer cells and T cells—that was present in blood samples taken before surgery. Patients with this signature were far more likely to have a leak afterwards. In technical terms, a simple logistic regression model using these 11 features correctly separated high‑risk from low‑risk patients with strong accuracy, with an area under the receiver operating characteristic curve of 0.81. When the new immune‑based signature was combined with the best existing surgical risk score, performance improved even further. The pattern the authors saw pointed to an immune system tilted toward excessive cytotoxic activity, chronic inflammation, and weakened regulation—conditions that may impair tissue repair, make surgical joins more fragile, and reduce control of secondary infections.
What this could mean for care
Although small and still in need of independent confirmation, the study suggests that a single preoperative blood draw could one day help flag patients who are biologically primed for a poor response to pancreatic surgery. Knowing this in advance might influence decisions about how to repair the pancreas, how closely to monitor the patient, whether to use additional protective measures, or even when to operate. It also opens the door to tailored preparation plans that strengthen the immune system or gently rebalance it before the operation. In plain terms, the authors conclude that the immune system’s fingerprint—measured before surgery—may offer an early warning of a dangerous leak, giving doctors a precious chance to act before trouble starts.
Citation: Garnier, J., Bellan, G., Palen, A. et al. Preoperative lymphocyte signature predicts pancreatic fistula after pancreatoduodenectomy. Commun Med 6, 158 (2026). https://doi.org/10.1038/s43856-026-01422-y
Keywords: pancreatic surgery, postoperative pancreatic fistula, immune profiling, machine learning, surgical complications