Clear Sky Science · en
Neoadjuvant transarterial chemoembolization with tyrosine kinase and immune checkpoint inhibitors improves survival from resectable hepatocellular carcinoma in a multicenter, retrospective study (GUIDANCE002)
Why this matters for people with liver cancer
Many people are diagnosed with liver cancer only after it has grown large or spread within the liver, making treatment especially challenging. This study looks at whether giving a powerful combination of treatments before surgery can help people with more advanced, but still removable, liver tumors live longer. The findings offer hope for better outcomes, but also highlight serious risks that patients and doctors must weigh carefully.
A tough-to-treat cancer
Hepatocellular carcinoma is the most common form of primary liver cancer, and about 70% of patients are first diagnosed at intermediate or advanced stages, when several tumors are present or major blood vessels may be involved. In China and some other countries, surgeons sometimes remove parts of the liver even at these later stages if enough healthy liver can be left behind. While such operations can prolong life, many patients see their cancer return within a few years, so researchers are searching for ways to improve long-term control of the disease.
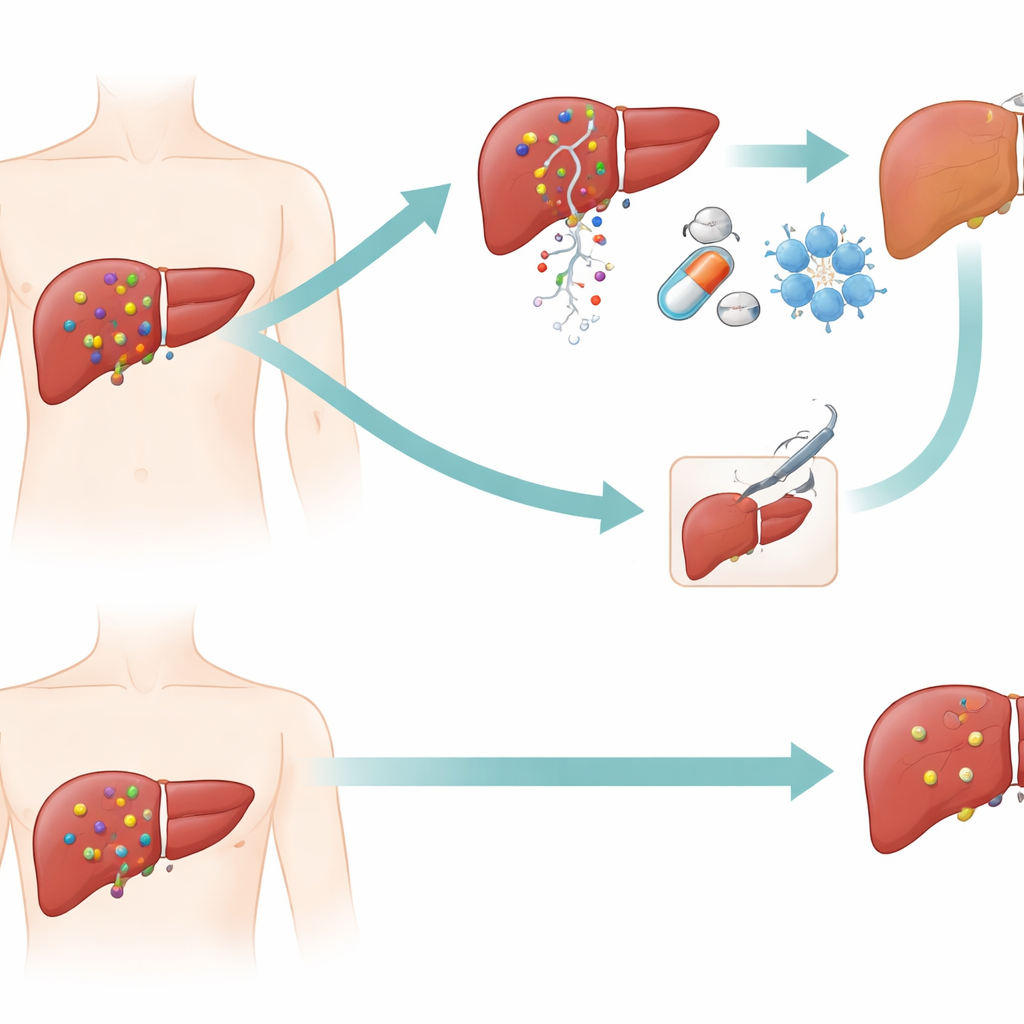
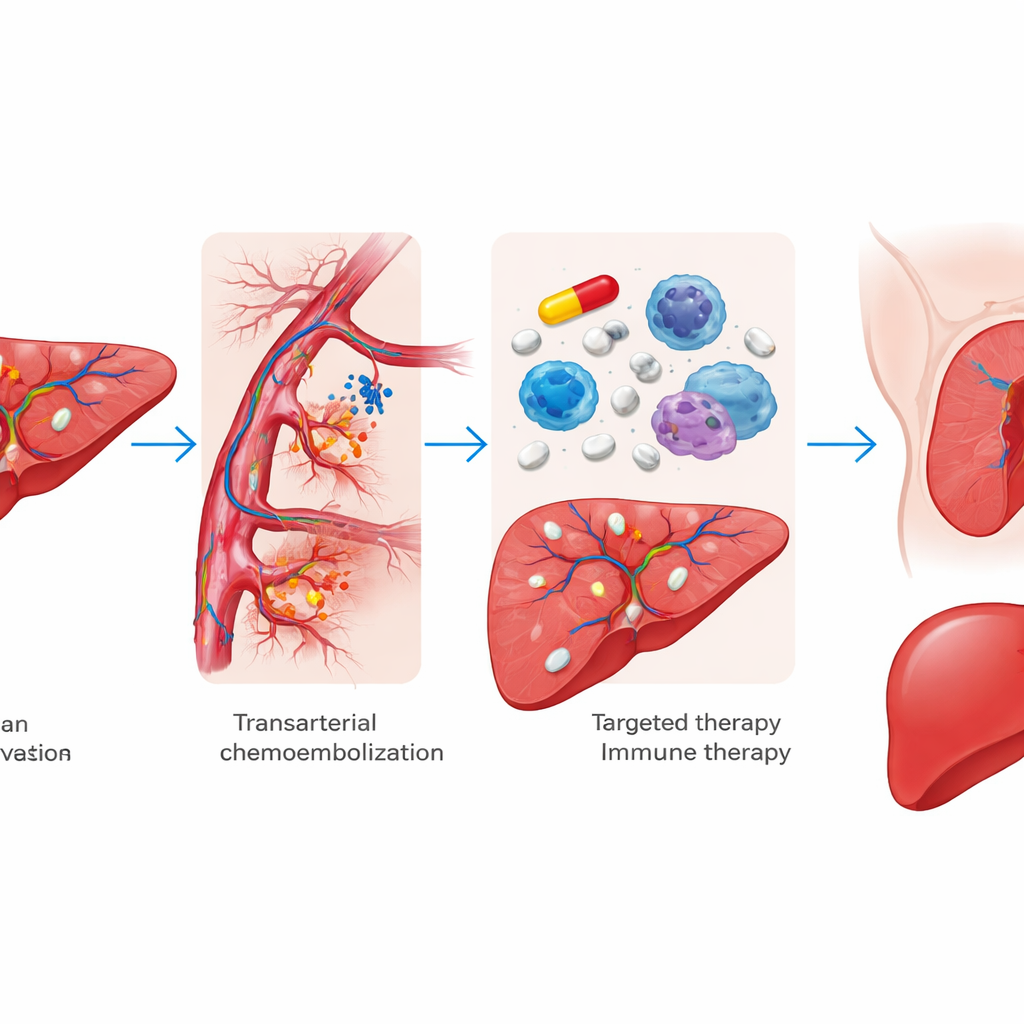
A three-part attack before surgery
The team examined a treatment strategy they call “neoadjuvant triple therapy,” meaning three treatments given before surgery. First, doctors deliver chemotherapy directly into the arteries feeding the liver tumors while blocking those blood vessels, starving the cancer of its blood supply. Next, patients receive tablets that block growth signals inside cancer cells (targeted drugs known as tyrosine kinase inhibitors). Finally, they receive immune checkpoint inhibitors, drugs that help the body’s own immune system recognize and attack tumor cells. The idea is to shrink or weaken tumors throughout the liver before surgeons attempt to remove all visible disease.
Comparing pre-treatment plus surgery with surgery alone
Researchers reviewed data from 583 adults treated at 20 hospitals in China between 2019 and 2023, all of whom had intermediate or advanced but still operable liver cancer. Of these, 378 went straight to surgery, while 205 received triple therapy first. About half of the triple-therapy group eventually had surgery; the others continued with local or drug treatments, or became ineligible for surgery because their tumors progressed. Using several statistical methods to make the groups as comparable as possible, the authors found that patients who received triple therapy before surgery lived longer overall and went longer without their disease returning or worsening than those who had surgery alone.
Benefits and trade-offs of the intensive approach
Patients who had surgery after triple therapy had especially strong results: higher three-year survival, longer time without relapse, and more complete or near-complete destruction of tumor tissue under the microscope. The triple therapy turned out to be particularly valuable for patients with more advanced disease, including those in a more serious stage group. However, this aggressive strategy came with clear downsides. About one in three patients on triple therapy suffered severe side effects such as high blood pressure, rash, or abdominal problems, and people who then underwent surgery had higher rates of serious postoperative issues like liver failure, bile leakage, and fluid buildup in the abdomen. A small group—16 patients—lost their chance for surgery altogether when their cancer advanced during the pre-surgery treatment period.
Who is most likely to benefit
The study also explored which patients might or might not need such an intensive plan. Certain warning signs, such as very high levels of the blood marker alpha-fetoprotein and invasion of large blood vessels, were linked both to worse survival and to a greater risk that tumors would progress so much during triple therapy that surgery was no longer possible. On the other hand, people with a single tumor, no major blood vessel invasion, and better liver function sometimes did just as well with immediate surgery, and might be spared the extra risk and cost of triple therapy. The authors stress that decisions should be made by a multidisciplinary team familiar with complex liver surgery and advanced cancer care.
What this means for patients
In plain terms, this large real-world study suggests that hitting liver cancer hard before surgery—with targeted drugs, immune therapy, and artery-blocking chemotherapy—can help many patients with more advanced but still operable disease live longer and stay free of cancer for more time than surgery alone. At the same time, the approach brings more side effects, more surgical complications, and a small but real risk of losing the window for curative surgery. The authors conclude that neoadjuvant triple therapy is a promising option for carefully selected patients, but that it should be used thoughtfully, with close monitoring and clear discussions about the balance between its potential survival benefits and its considerable risks.
Citation: Yang, DL., Qin, C., Peng, N. et al. Neoadjuvant transarterial chemoembolization with tyrosine kinase and immune checkpoint inhibitors improves survival from resectable hepatocellular carcinoma in a multicenter, retrospective study (GUIDANCE002). Commun Med 6, 139 (2026). https://doi.org/10.1038/s43856-025-01303-w
Keywords: liver cancer, hepatocellular carcinoma, neoadjuvant therapy, immunotherapy, chemoembolization