Clear Sky Science · en
Axicabtagene ciloleucel in combination with rituximab for refractory large B cell lymphoma: the phase 2, single-arm ZUMA-14 trial
Why this new lymphoma treatment matters
For people with an aggressive blood cancer called large B cell lymphoma, standard chemotherapy does not always work, and even powerful cell-based treatments can lose their punch over time. This study tested a new strategy: combining a customized immune cell therapy with a long‑used antibody drug to see if attacking the cancer on two fronts could keep it from coming back and do so without adding unsafe side effects.
Two medicines teaming up against one cancer
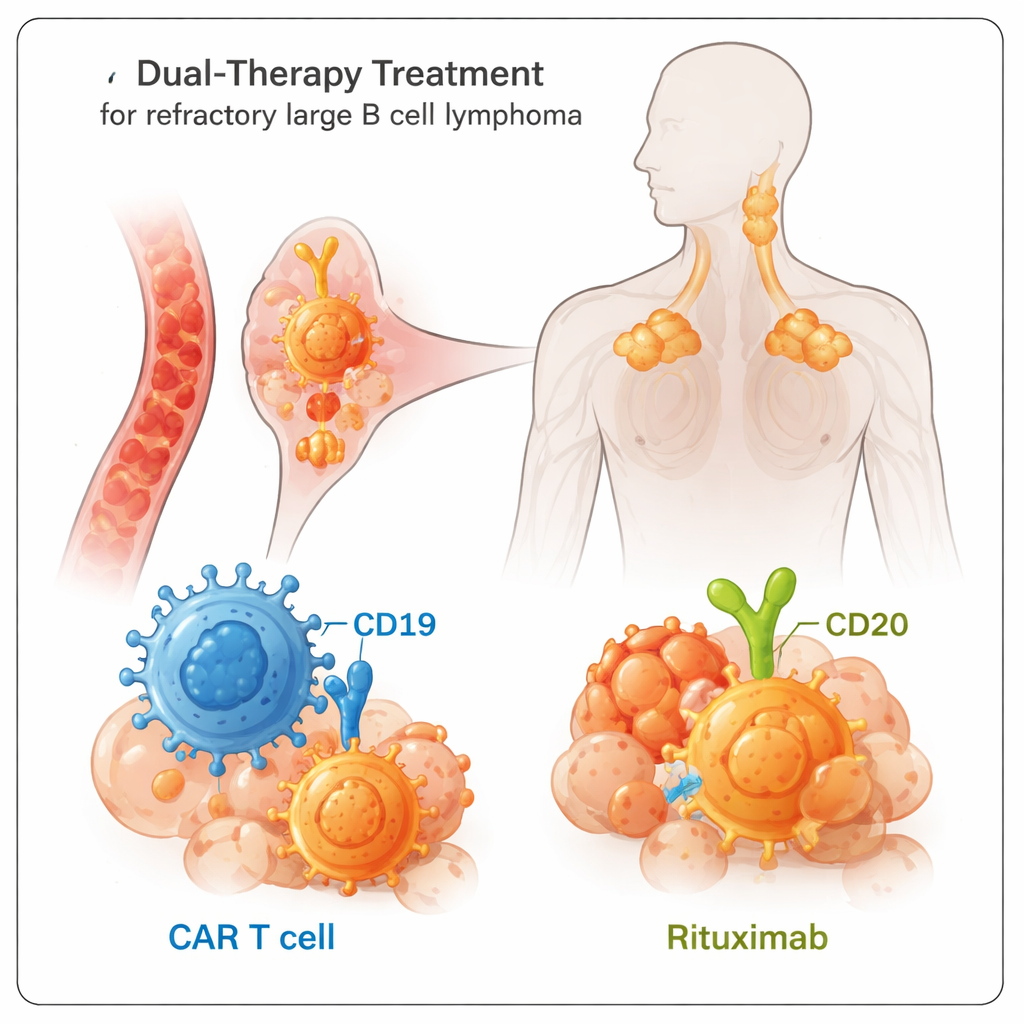
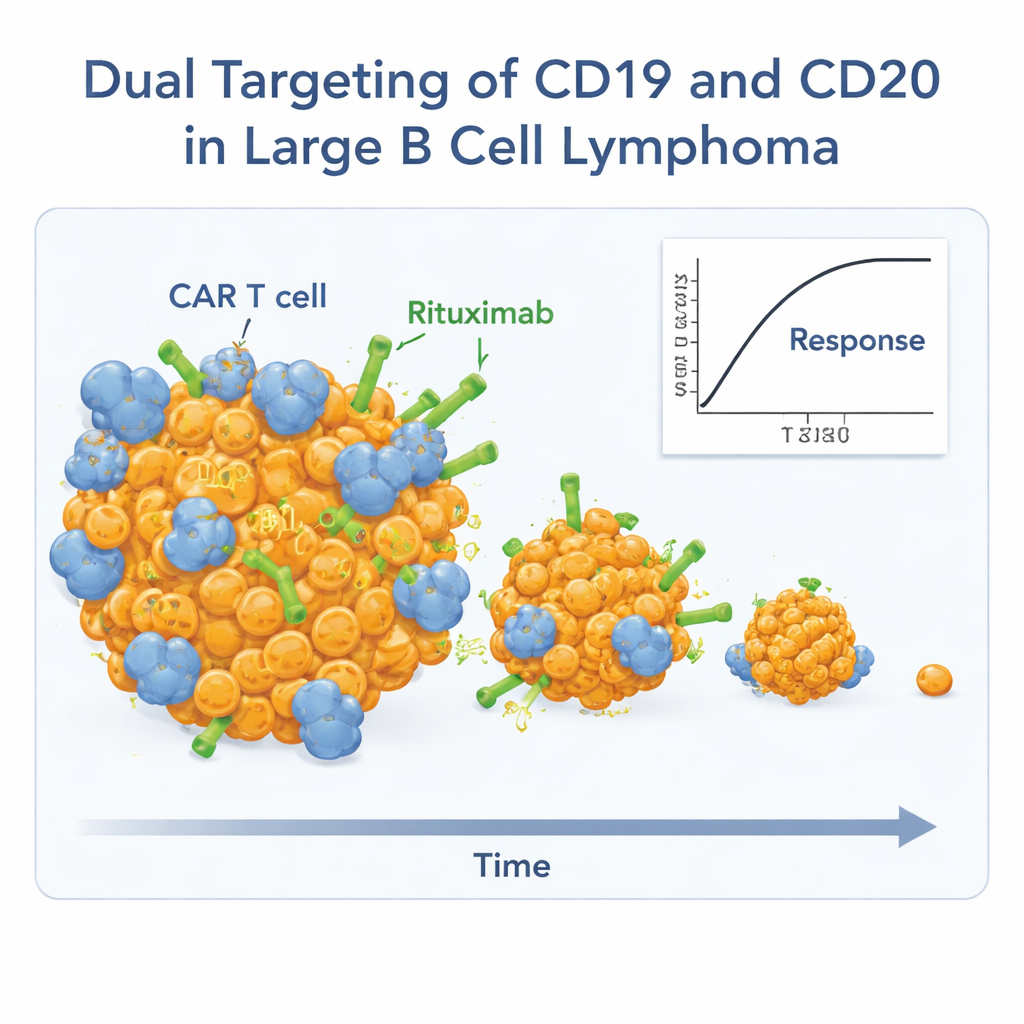
The trial focused on adults whose lymphoma had not responded to prior treatments, a group that usually faces poor outcomes. All participants received axicabtagene ciloleucel, or axi‑cel, a type of CAR T cell therapy made from their own T cells engineered to hunt cells carrying a marker called CD19. On top of this, they were given rituximab, an antibody drug that locks onto a different marker on the same cancer cells, called CD20. The idea was simple but powerful: by hitting two targets on the lymphoma cells at once, the cancer would have a harder time “escaping” by dropping one of these markers.
Stronger and longer‑lasting responses
Among the 26 people who received both treatments, nearly 9 out of 10 saw their tumors shrink, and almost three‑quarters had no detectable signs of cancer on scans, known as a complete response. Many of these deep responses were not just quick flashes of success. At just over two years of follow‑up, almost half of the participants still had ongoing responses. The median length of response was about 26 months, and the typical time people lived without their disease worsening was almost two years. Overall survival was not yet reached at the time of analysis, meaning that more than half of the patients were still alive.
Side effects remain serious but manageable
Because CAR T therapies rev up the immune system, they can cause intense side effects, especially a reaction called cytokine release syndrome and temporary brain‑related symptoms. In this study, nearly everyone had some level of immune reaction, but importantly, no one developed the most severe grades of cytokine release syndrome, and serious nerve problems occurred in about 15% of patients; all of these episodes eventually resolved. Low blood counts and infections were common, as expected, but adding rituximab did not appear to make these complications clearly worse compared with earlier studies of axi‑cel alone. Two patients developed a second blood cancer, a rare but known long‑term risk with powerful immune therapies.
Clues to who benefits most
Researchers also probed the biology behind success and failure of the combination. People whose blood showed higher levels of CAR T cells and rituximab exposure tended to be those with the strongest and most durable responses. Very few patients had normal B cells—the type of cell that turns cancerous in this disease—for a full year after treatment, showing that the therapy remained active. Tumor samples taken before treatment suggested that cancers already rich in certain immune cells, like natural killer cells and memory‑type T cells, were more likely to stay in long‑term remission. Blood tests for fragments of tumor DNA also hinted that early detection of even tiny amounts of remaining disease could predict later relapse.
What this means going forward
For patients whose lymphoma has resisted multiple rounds of treatment, the combination of axi‑cel and rituximab delivered high response rates and many long‑lasting remissions without introducing unexpected safety problems. While the trial was small and had no direct comparison arm, its results support the idea that hitting cancer cells through both CD19 and CD20 can help prevent the tumor from slipping past a single‑target therapy. This dual‑target approach is now inspiring next‑generation cell therapies designed to build the same two‑pronged attack directly into a single product, with the hope of making powerful, durable treatments more convenient and widely available.
Citation: Strati, P., Leslie, L., Shiraz, P. et al. Axicabtagene ciloleucel in combination with rituximab for refractory large B cell lymphoma: the phase 2, single-arm ZUMA-14 trial. Nat Cancer 7, 304–315 (2026). https://doi.org/10.1038/s43018-025-01102-1
Keywords: CAR T cell therapy, large B cell lymphoma, rituximab, dual antigen targeting, immunotherapy resistance