Clear Sky Science · en
A deep learning radiopathomic signature predicts recurrence risk of hepatocellular carcinoma after hepatectomy
Why this matters for people with liver cancer
Liver cancer is among the deadliest cancers worldwide, and even when surgeons remove the visible tumor, many patients see the disease return within just a few years. This study introduces an artificial intelligence tool that combines medical scans and microscope images of tumors to better forecast who is likely to experience a comeback of hepatocellular carcinoma, the most common form of liver cancer. Such predictions could help doctors tailor follow-up care and extra treatments, aiming to prevent recurrence and extend patients’ lives.
Seeing the whole tumor, inside and out
Doctors typically rely on CT scans, blood tests, and basic pathology reports to estimate recurrence risk after liver surgery. Each of these tools looks at the tumor from a different angle, but none fully captures its complexity. CT images show the tumor’s overall shape, blood supply, and relationship to the liver, while microscope slides reveal how aggressive the cancer cells look and how they interact with surrounding tissue. The researchers reasoned that a computer system that “looks” at both levels together—organ-wide scans and cell-level images—might recognize patterns that humans miss and therefore more accurately predict whether the cancer will return.
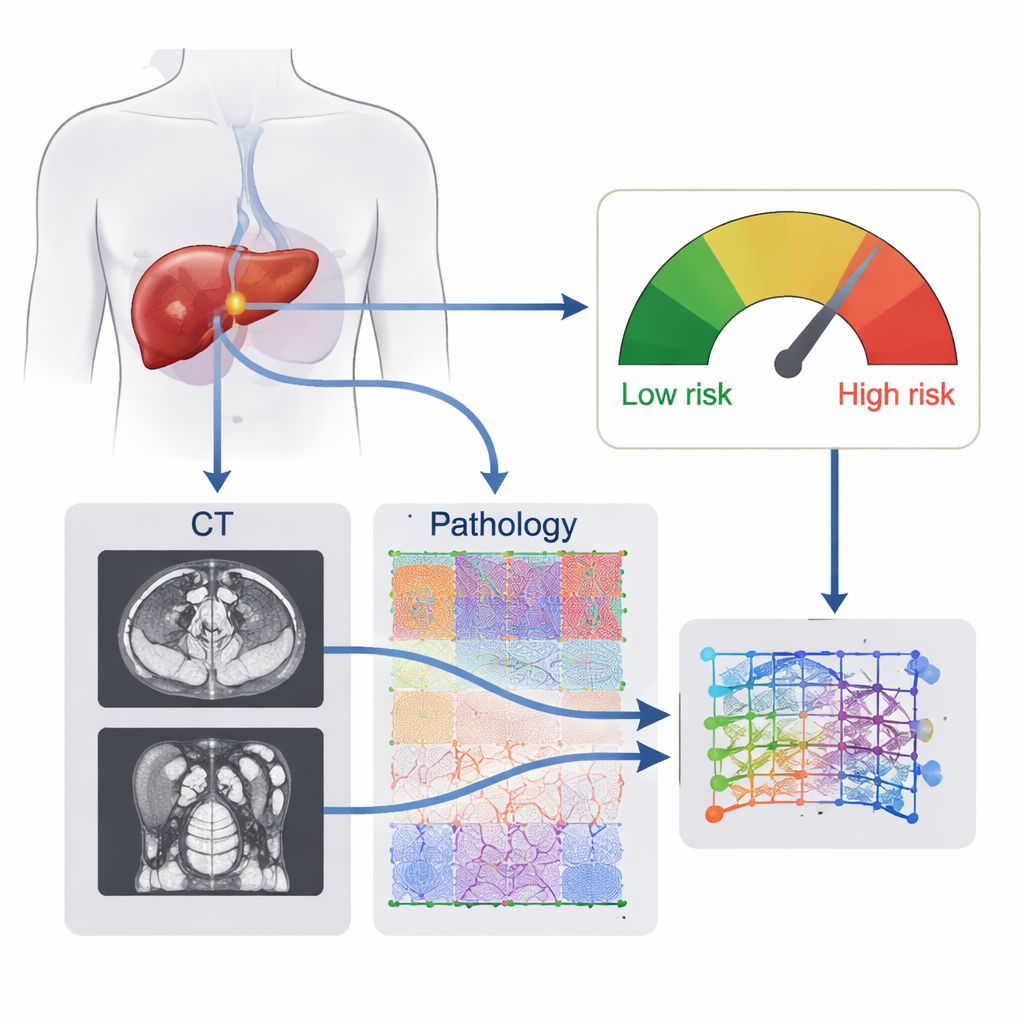
A combined digital fingerprint of the tumor
The team developed what they call a deep learning radiopathomic (DLRP) signature, essentially a digital fingerprint of each patient’s tumor built from two data sources. First, a neural network automatically outlined tumors on preoperative CT scans and learned subtle image features linked to recurrence. Second, another network analyzed whole-slide images of routine hematoxylin-and-eosin–stained tissue, breaking them into thousands of small patches and learning which microscopic patterns mattered most. A fusion module then wove the CT features and pathology features together into a single risk score that reflects the tumor’s behavior rather than any single visible trait.
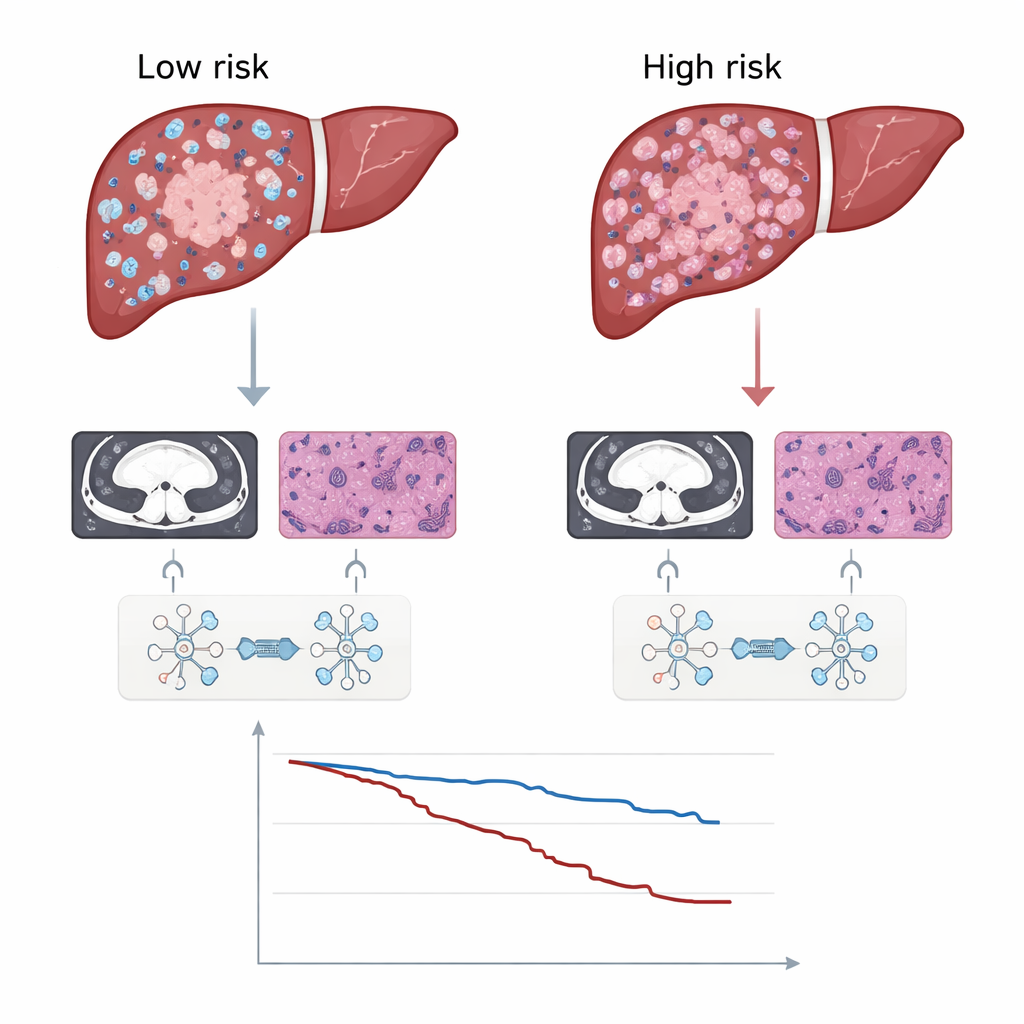
Testing the score in real patients
The researchers applied this system to 599 people who had surgery for hepatocellular carcinoma at four hospitals, dividing them into training and independent test groups. Across all test sets, the DLRP signature predicted recurrence-free survival better than models that used only CT, only pathology, standard clinical variables such as tumor size and blood markers, or the widely used Barcelona Clinic Liver Cancer stage. Patients with high DLRP scores had a markedly greater chance of tumor coming back and also shorter overall survival. Importantly, this held true across many subgroups, including those with small versus large tumors, single versus multiple tumors, and with or without cirrhosis, suggesting that the score captures core aspects of tumor aggressiveness.
Guiding extra treatment and revealing biology
Beyond prediction, the score helped identify which patients might benefit from an additional procedure called postoperative adjuvant transarterial chemoembolization (PA-TACE), in which chemotherapy mixed with an oily contrast agent is injected into the liver’s blood supply. Among all patients combined, those who received PA-TACE tended to stay free of recurrence longer. But when the group was split by the DLRP signature, the benefit was concentrated almost entirely in the high-risk patients; low-risk patients saw no clear advantage, implying they could safely avoid the burdens of extra therapy. The team also explored why high-risk tumors behave worse by linking the DLRP scores to genetic data from The Cancer Genome Atlas. High scores were associated with activation of the Wnt/β-catenin pathway, known to drive tumor growth and resistance to immunotherapy, and with fewer cancer-fighting immune cells, especially CD8 T cells, infiltrating the tumor.
What this means for future liver cancer care
For a layperson, the takeaway is that computers can now blend X-ray–like images and microscope views to produce a single number that tells how likely a liver cancer is to come back after surgery. This study shows that such a number can outperform traditional staging systems and may help decide who truly needs extra treatment and more intensive follow-up. While the tool still needs prospective testing in broader patient populations, including those whose liver disease was not caused by hepatitis B, it points toward a future in which treatment plans are shaped by rich, multi-layered portraits of each person’s tumor rather than by size and stage alone.
Citation: Wang, G., Chen, W., Liang, Z. et al. A deep learning radiopathomic signature predicts recurrence risk of hepatocellular carcinoma after hepatectomy. Commun Biol 9, 295 (2026). https://doi.org/10.1038/s42003-026-09571-5
Keywords: hepatocellular carcinoma, liver cancer recurrence, deep learning, medical imaging, tumor microenvironment