Clear Sky Science · en
Treatment adherence and clinical outcomes of osimertinib in minority patients with advanced EGFR mutated NSCLC
Why this cancer story matters
Lung cancer is still the number-one cancer killer in the United States, but powerful new pills have transformed the outlook for some patients. One of the most important of these drugs is osimertinib, a daily tablet that targets tumors with specific DNA changes. Yet most of the data proving its benefits come from clinical trials that enrolled very few Black and Hispanic patients. This study asks a pressing question: when people from different racial and ethnic backgrounds receive the same modern drug at a safety-net cancer center, do they all live equally long?
A closer look at a targeted lung cancer pill
Doctors at the Montefiore Einstein Comprehensive Cancer Center in the Bronx reviewed the records of 174 people with advanced non-small cell lung cancer whose tumors carried EGFR mutations—precise DNA alterations that make them eligible for osimertinib. Unlike many clinical trials, this group reflected the diversity of the surrounding community: about one-third were Hispanic, nearly one-third were non-Hispanic Black, one-quarter were non-Hispanic White, and the rest were Asian. Most had never smoked and nearly all had a similar type of lung cancer called adenocarcinoma. Osimertinib was used either as the very first treatment or after other therapies had failed.
Who gets the drug and who can afford it
The researchers examined practical barriers that often drive health gaps, such as income, insurance, and the high cost of brand-name cancer medicines. Many Black and Hispanic patients lived in lower-income neighborhoods and relied on Medicaid. On paper, the drug was extremely expensive—about $16,700 per month—but insurance coverage and assistance programs cut the average out-of-pocket cost to under $60, with a median cost of zero dollars. Pharmacy refill records suggested that most patients, regardless of race or ethnicity, were able to take the pill as prescribed more than 80 percent of the time, a common standard for good adherence. In other words, at this center, access to the drug and the ability to stay on it looked broadly similar across groups.
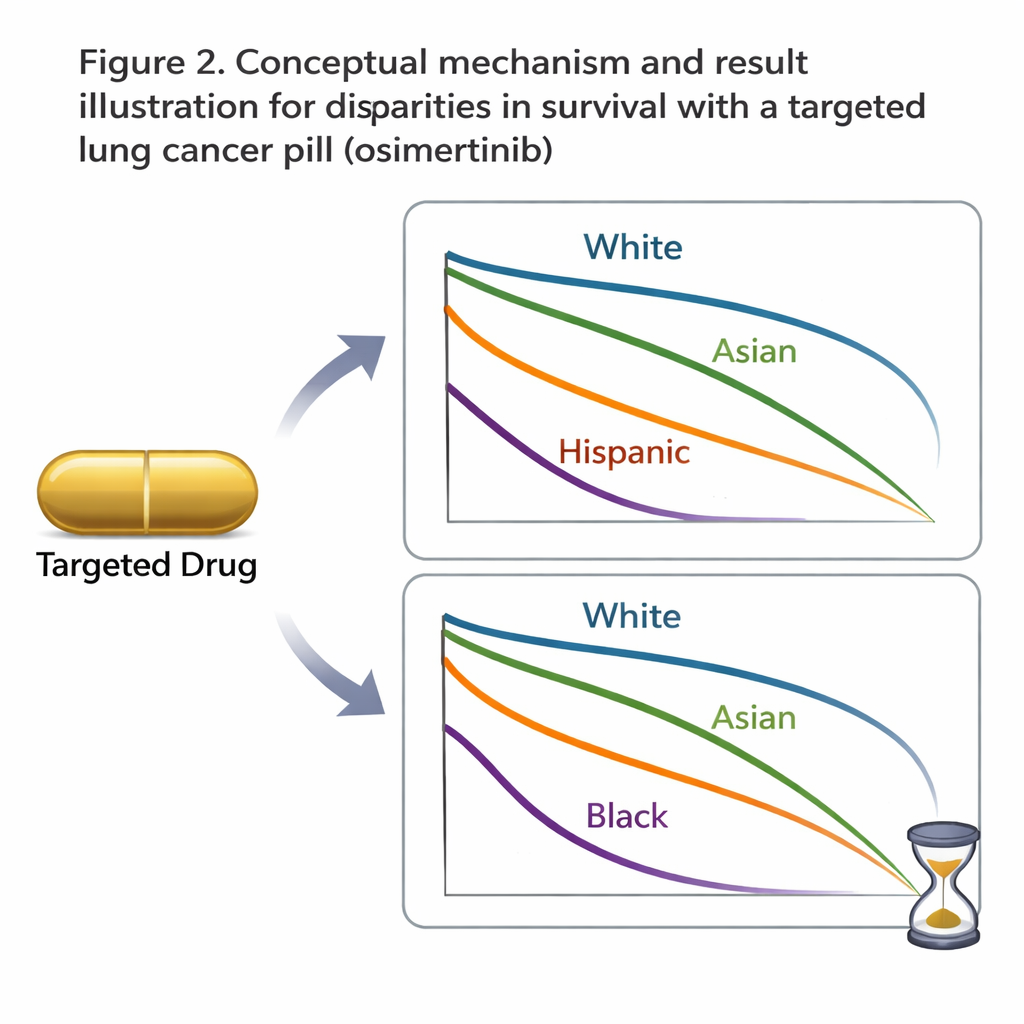
When equal treatment does not mean equal outcomes
Even with comparable access and adherence, survival told a different story. Overall, patients lived a median of about 33 months after starting osimertinib. Non-Hispanic White patients had the longest median survival at just over 40 months. Non-Hispanic Black patients lived a median of only about 22 months, while Hispanic and Asian patients fell in between. When the team used statistical models that accounted for age, sex, body weight, tumor mutation type, and how sick patients were at the start of treatment, being non-Hispanic Black was still linked to a significantly higher risk of death. This survival gap was even more striking among people who received osimertinib as their very first treatment, suggesting that the difference was not simply due to what therapies they had tried before.
Looking beyond income and insurance
To see whether money or coverage fully explained these patterns, the investigators tested the impact of neighborhood income, insurance type, side effects, and how faithfully patients took their pills. None of these factors, on their own, could account for the shorter survival among Black patients. The authors point instead to a tangle of possible biological and health-system reasons. Osimertinib is broken down in the body by liver enzymes that vary among individuals and populations; some genetic variants, more common in Black people, may clear the drug faster, effectively lowering the dose. Higher average body weight in Black and Hispanic patients could also dilute a one-size-fits-all pill. Tumors themselves may differ in additional mutations that were not routinely measured. And unrecorded differences in other illnesses or in follow-up care after the cancer worsens could further widen the gap.
What this means for patients and care
For a lay reader, the key message is sobering but actionable: giving everyone the same advanced cancer drug is not enough to guarantee the same chance of survival. In this real-world study, Black patients with EGFR-mutated lung cancer died sooner than their White peers despite similar access to a high-cost, highly effective pill. The authors argue that to close this gap, cancer research and clinical trials must include many more minority patients, dosing may need to be personalized rather than fixed, and doctors must probe both genetic differences in how drugs are handled and subtle inequalities in ongoing care. Only by understanding and addressing these layered causes can precision oncology live up to its promise for all communities.
Citation: Lee, M., Song, J., Miao, E. et al. Treatment adherence and clinical outcomes of osimertinib in minority patients with advanced EGFR mutated NSCLC. npj Precis. Onc. 10, 90 (2026). https://doi.org/10.1038/s41698-025-01259-z
Keywords: lung cancer, targeted therapy, health disparities, osimertinib, EGFR mutation