Clear Sky Science · en
Pharyngeal electrical stimulation for postextubation dysphagia after stroke: a randomized trial on hospitalization costs from a health insurance perspective
Why this matters for patients and payers
When someone survives a severe stroke and needs a breathing tube, they often wake up with great difficulty swallowing. This problem, called trouble swallowing, can lead to food or saliva going into the lungs, pneumonia, long stays in intensive care, and very high hospital bills. This study asks a simple but important question: can a brief, targeted stimulation of the throat both help patients and reduce the chance of extremely expensive hospital stays from a health insurer’s point of view?
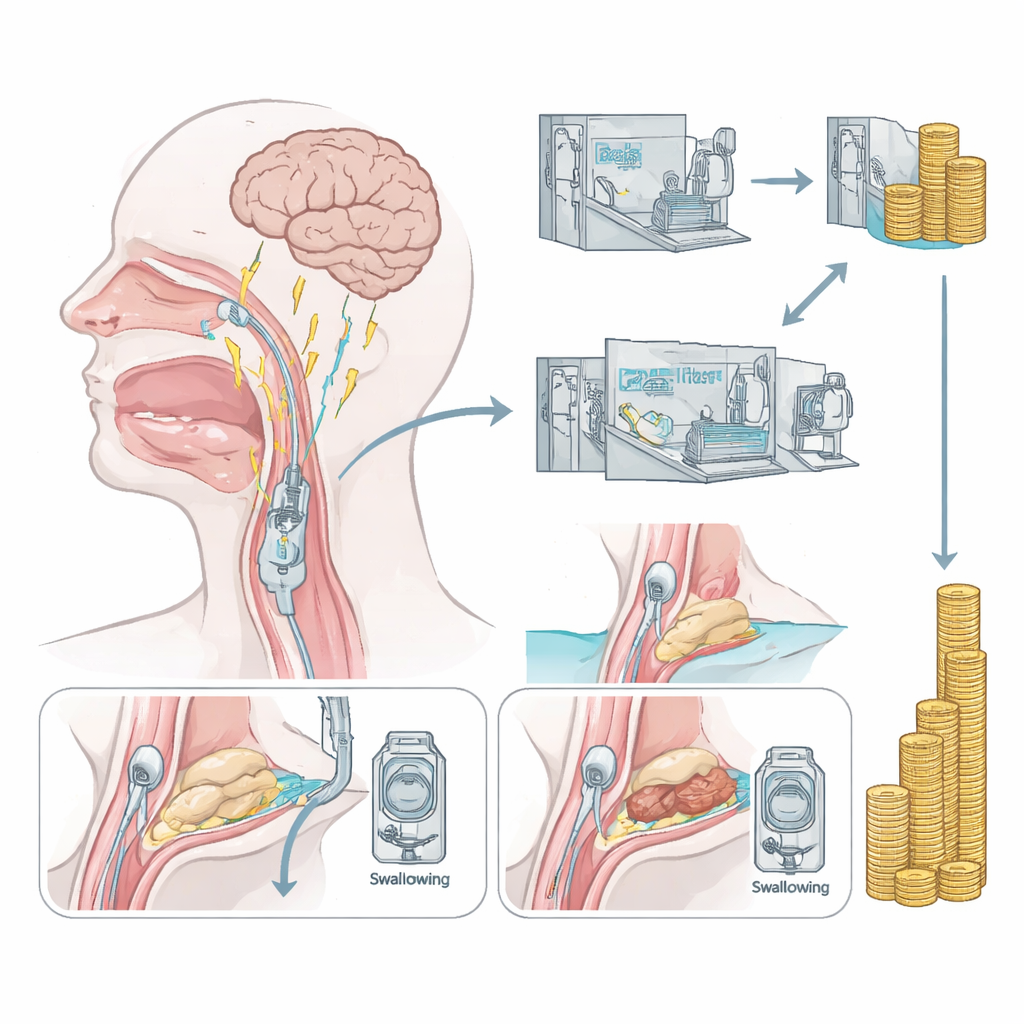
A new way to help the throat recover
Today, most treatments for swallowing problems after stroke focus on working around the difficulty: changing food textures, careful mouth care, or feeding through tubes. They rarely restore the swallowing function itself. Pharyngeal electrical stimulation (PES) takes a different approach. A thin catheter is gently passed through the nose so that small electrical pulses can be delivered to the lining of the throat for ten minutes a day over three days. Earlier research showed that this stimulation can reshape activity in brain areas that control swallowing and can help very severely affected patients come off tracheostomy tubes. But it was still unclear whether this approach would also influence the overall costs of hospital care.
How the study was set up
The authors performed a secondary analysis of a previous randomized trial in a university stroke center in Germany. Sixty adults who had suffered an acute stroke, needed mechanical ventilation, and had severe swallowing problems right after their first removal of the breathing tube were enrolled. All patients received the same intensive stroke and swallowing care. Half were randomly assigned to receive PES, and half had a sham procedure in which the catheter was placed but no stimulation was delivered. Neither the bedside teams nor the people judging outcomes knew who was in which group. For each patient, the researchers later calculated what the hospital was allowed to bill German statutory health insurers, using the 2025 Diagnosis Related Groups (DRG) rules—a standardized payment system that bundles diagnoses, procedures, ventilation time, and other factors into flat-rate reimbursements.
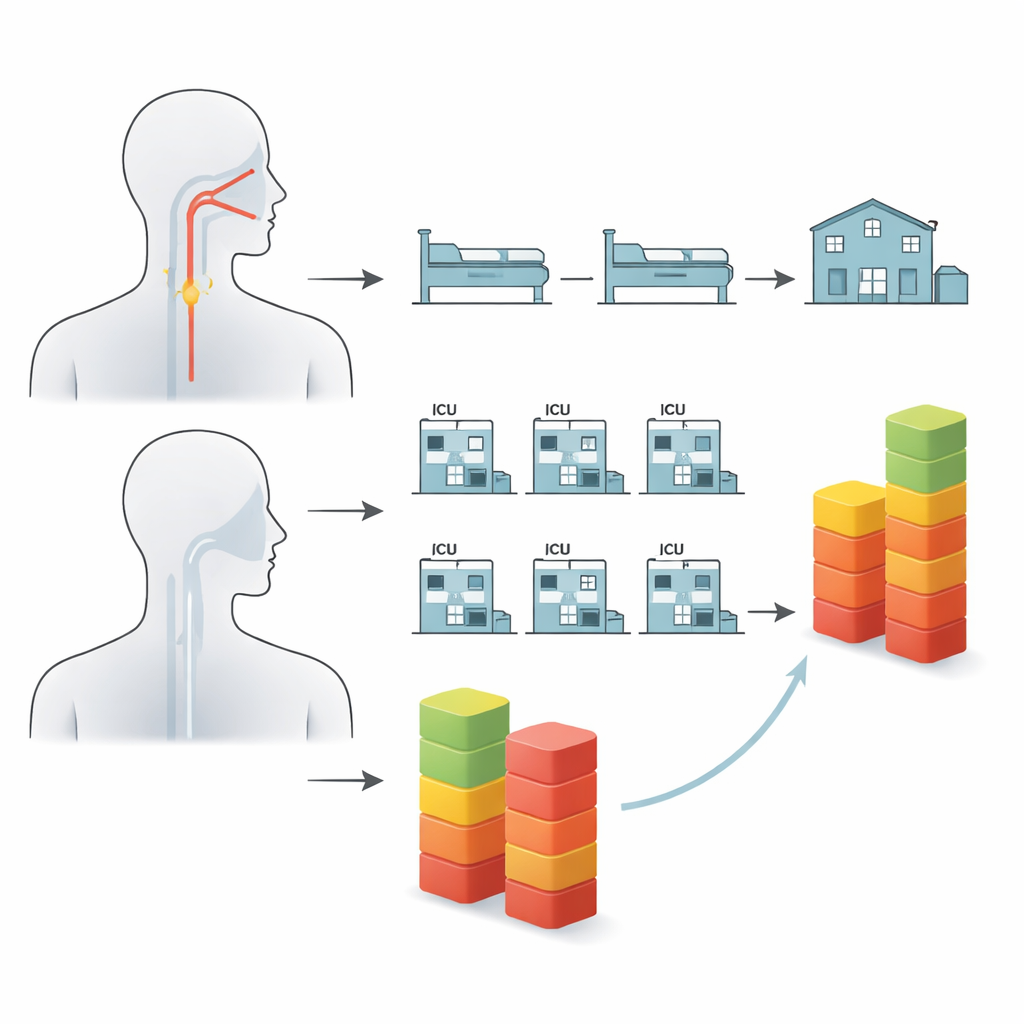
What the bills revealed
On average, patients in the sham group generated higher hospital payments than those who received PES. The mean billed amount in the control group was about €22,400, compared with roughly €18,100 in the PES group, and the middle value (the median) was also higher in the control group. Statistically, however, this difference did not quite reach the accepted threshold for calling it a clear effect, which the authors attribute in part to the modest sample size and the fact that the original trial had been designed to study reintubation, not costs. The pattern of the bills, rather than the average alone, turned out to be especially revealing.
The story behind the rare, very expensive cases
When the researchers looked more closely at the spread of costs, three patients in the sham group stood out as extreme outliers, each with bills greater than about €50,600, and one exceeding €57,800. None of the patients who received PES reached such levels; the highest reimbursement in that group was about €35,300. The three very costly control patients had particularly long durations of mechanical ventilation (on average more than 700 hours in total), much longer hospital stays, and all developed pneumonia, even though they were not more burdened by other illnesses than their peers. This suggests that complications related to breathing support and chest infections, rather than underlying disease alone, drove the runaway costs—and that PES, by improving throat sensation and secretion handling, may have helped prevent such spirals in its group.
What this could mean for health systems
From an insurer’s perspective, a handful of very complex cases can dominate total spending for stroke care. In this study, PES did not show a statistically proven reduction in average hospital costs, and the price of the stimulation equipment itself was not included in the calculations. Still, the absence of extreme high-cost cases in the PES group is striking and fits with earlier evidence that this technique can reduce the need for reintubation and shorten time in intensive care. The authors caution that the findings are exploratory and limited to the German payment system, but they argue that larger, dedicated economic trials are now warranted. If future studies confirm that PES reliably lowers the risk of such costly complications, health insurers may find it financially worthwhile to cover the treatment, in addition to its potential benefits for patients’ safety and recovery.
Citation: Labeit, B., Jung, A., von Itter, J. et al. Pharyngeal electrical stimulation for postextubation dysphagia after stroke: a randomized trial on hospitalization costs from a health insurance perspective. Sci Rep 16, 8556 (2026). https://doi.org/10.1038/s41598-026-43591-9
Keywords: stroke, swallowing problems, pharyngeal electrical stimulation, intensive care, healthcare costs