Clear Sky Science · en
Radar-based inspiratory-to-expiratory time ratio estimation: a validation study
Why watching the breath matters
Every time we breathe in and out, our bodies reveal clues about our health. Doctors usually count how many breaths we take per minute, but the detailed timing of each breath—how long we inhale versus exhale—can flag problems in the lungs, heart, or brain sooner and more precisely. Today, measuring these patterns typically means attaching wires, belts, or sticky electrodes to the body, which can be uncomfortable, restrict movement, and are hard to keep on for days at a time. This study asks a simple but powerful question: can a small radar device quietly placed near the bed track these intricate breathing details just as well, without touching the patient at all?

A new way to listen to breathing
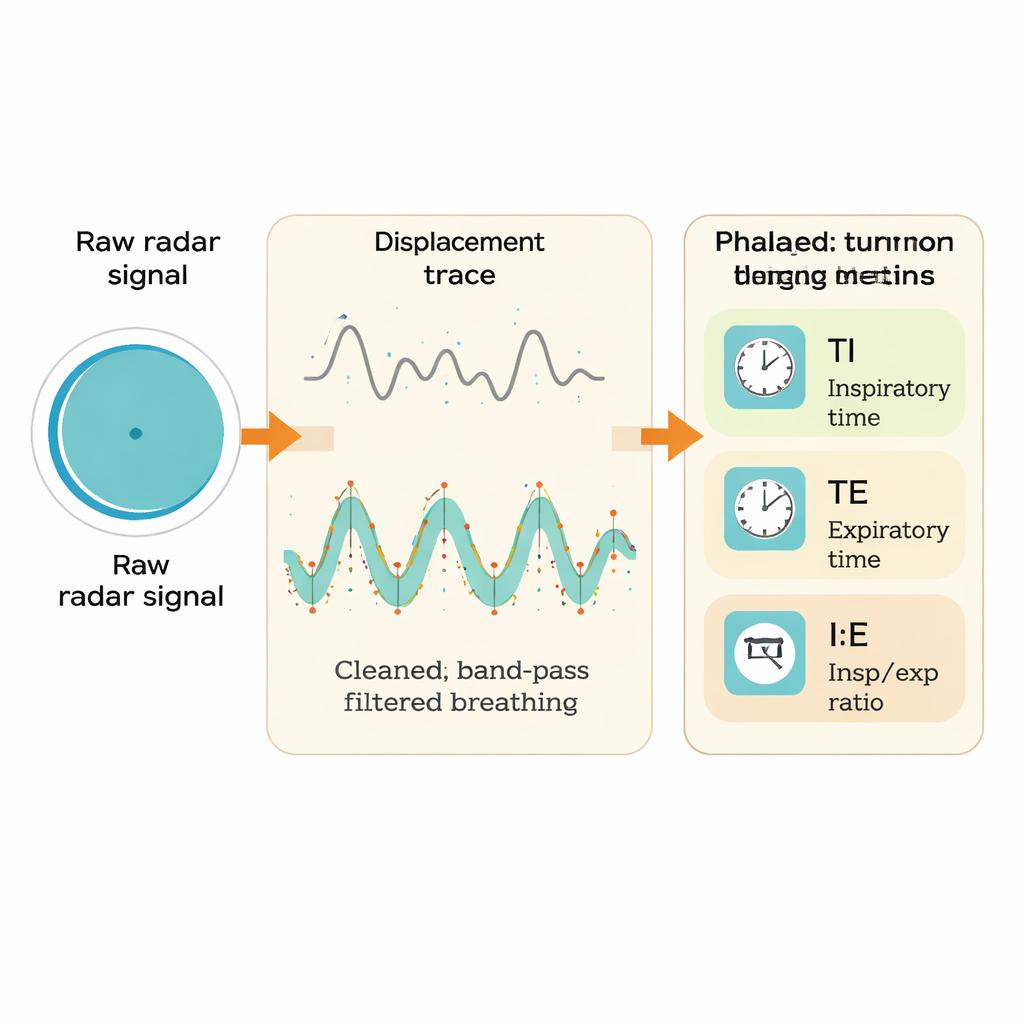
The researchers focused on four key breathing measures: the respiratory rate (how many breaths per minute), the time spent breathing in (inspiratory time), the time spent breathing out (expiratory time), and the ratio between the two. That ratio, known to doctors as the I:E ratio, is particularly important in intensive care and ventilator settings, where it helps fine-tune how machines support a patient’s lungs. To avoid wires and contact sensors, the team used a compact radar system that sends harmless radio waves toward a person’s chest and reads back the tiny movements caused by breathing. In principle, this allows the system to work through clothing, blankets, and even a mattress, making it attractive for hospital wards, recovery rooms after surgery, and end-of-life care.
How the radar readings were checked
To find out how trustworthy the radar really is, the team compared it with an established, contact-based method called impedance pneumography. This reference system uses small electrodes on the chest to measure changes in electrical resistance as the lungs fill and empty with air. Thirty healthy volunteers lay quietly on a special tilt table while both devices recorded their breathing at the same time. The team then processed the radar signals step by step: first correcting hardware imperfections, then converting phase changes of the radio waves into chest motion, and finally filtering the data to isolate the gentle rise and fall of breathing. From both radar and reference signals, they identified the peaks and valleys that mark when inhalation ends and exhalation begins, allowing them to calculate the timing of each breath cycle over many two‑minute windows.
How well the contactless method performed
When they compared the two systems, radar did remarkably well. For breathing rate, the agreement was very strong: in more than 97 percent of time windows, the radar’s estimate stayed within two breaths per minute of the reference, with almost no systematic over‑ or underestimation. The more demanding timing measures showed slightly larger differences but still stayed within medically acceptable limits. On average, radar’s estimates of inhalation time were just a few hundredths of a second longer, and its exhalation times a little shorter, than those from the wired system. The ratio between inhalation and exhalation, which amplifies small timing errors, showed the weakest match but still fell inside predefined safety bounds for the vast majority of measurements. Advanced statistical tests designed to judge whether two methods can be treated as equivalent confirmed that, for all four breathing metrics, radar and the reference system were effectively interchangeable within these limits.
What the study could not yet show
Like any carefully controlled experiment, this work has boundaries. All volunteers were healthy adults lying calmly at rest, for relatively short periods, in a quiet lab environment. Real‑world patients often move, cough, talk, or experience pain and distress, all of which can distort signals. Subtle chest movements in very slow, shallow, or irregular breathing can also make it harder for radar to detect the exact start and end of each breath, especially when the motion is barely visible. The authors note that more advanced, data‑driven algorithms and longer recordings in realistic hospital and home settings will be needed to fully understand how the technology behaves in everyday clinical practice.
What this means for patients and caregivers
Despite these limitations, the study delivers an encouraging message: a small, contactless radar device can measure not only how often we breathe, but also how long we spend breathing in and out, with accuracy close to a well‑established wired system. For patients, this could mean less equipment on the skin, more freedom to move, and quieter, more dignified monitoring—especially in palliative care, post‑surgery recovery, and intensive care units. For clinicians, it opens the door to continuous, unobtrusive tracking of detailed breathing patterns that may signal trouble earlier than simple breath counts alone. In short, radar-based monitoring brings us a step closer to “invisible” vital sign tracking that keeps a close watch on patients while getting out of their way.
Citation: Trần, T.T., Oesten, M., Griesshammer, S.G. et al. Radar-based inspiratory-to-expiratory time ratio estimation: a validation study. Sci Rep 16, 8256 (2026). https://doi.org/10.1038/s41598-026-42517-9
Keywords: respiratory monitoring, radar sensing, breathing patterns, noncontact vital signs, inspiratory–expiratory ratio