Clear Sky Science · en
Difficult biliary cannulation among patients with compensated liver cirrhosis: predictors and impact on complications
Why this matters for people with liver disease
Many people with long‑standing liver disease eventually develop scarring, or cirrhosis, and often need a procedure called ERCP to relieve blocked bile ducts or treat gallstones. Although ERCP is done with a flexible tube and camera and is considered minimally invasive, it can still cause serious problems such as inflammation of the pancreas or bleeding. This study asks a simple but important question: when doctors have a hard time entering the bile duct in patients with compensated (early-stage) cirrhosis, how often does that difficulty lead to complications, and can we predict who is at risk?
Looking closely at a common procedure
To explore this, researchers in Egypt followed adults with compensated liver cirrhosis who were having their first ERCP and had never had their bile duct opening cut or altered before. Over two years, 131 such patients were enrolled; in 127 of them, the doctors were ultimately able to reach the bile duct, and these patients formed the main analysis group. The team recorded details before, during, and after the procedure: age and other illnesses, how the small opening in the intestine (the papilla) looked, whether there were pouches near it (duodenal diverticula), how many times the doctors tried to enter the duct, how long it took, and which advanced tools they needed to use.
When the bile duct is hard to enter
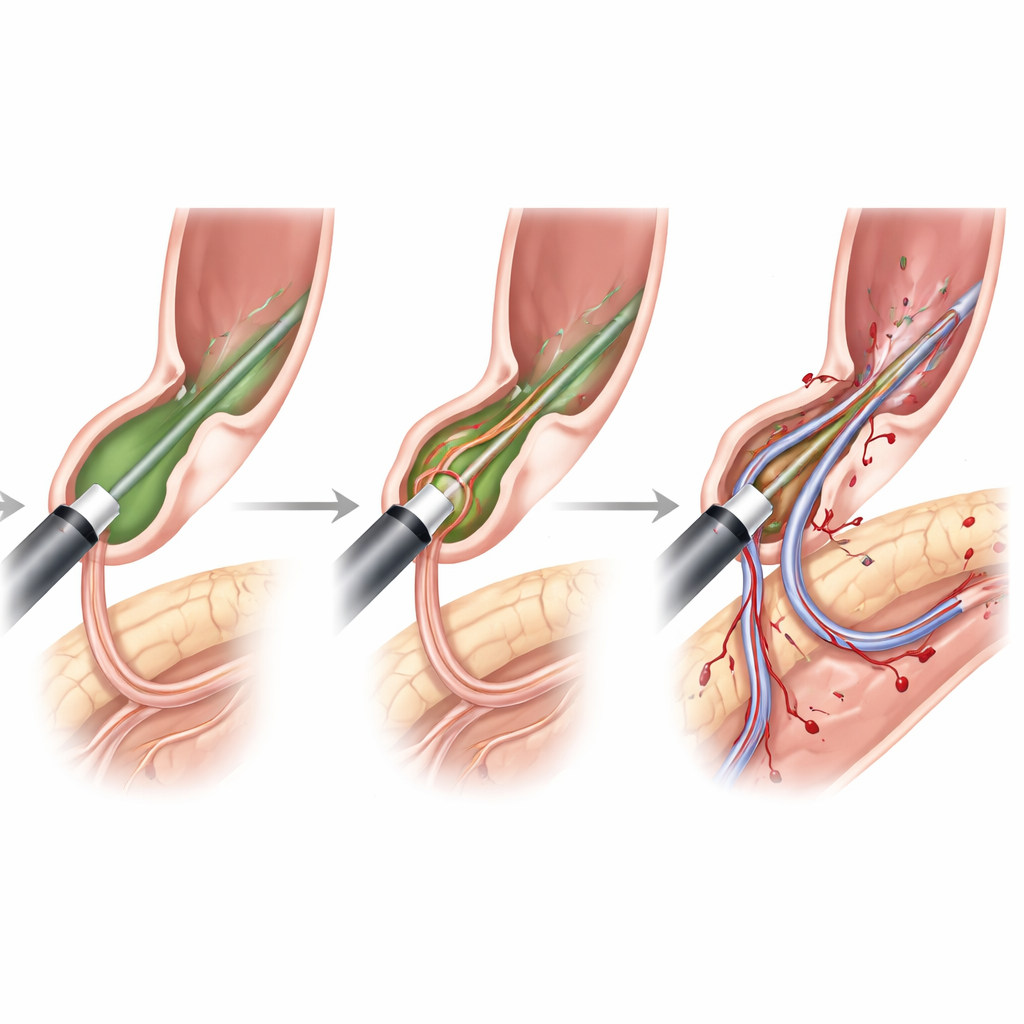
Using international guidelines, the authors labeled a case as "difficult biliary cannulation" when the endoscopist needed more than five contacts with the papilla, more than five minutes of trying, or repeatedly entered the pancreatic duct by mistake. By these standards, difficult cannulation occurred in nearly half of the cirrhotic patients (45.5%). Several features made the task harder. Older patients were more likely to fall into the difficult group. Certain papilla shapes—very small openings (type 2) or large, dangling ones (type 3)—were linked to more trouble, as was the presence of a diverticulum, a bulging pocket of the small intestine near the papilla. When doctors had to resort to a "precut" technique, using a cutting tool to open the papilla and reach the duct, difficulty was almost guaranteed.
Complications follow prolonged struggle
The overall success rate of entering the bile duct was high at almost 97%, but this came at a cost: 12.6% of patients developed short‑term complications. Inflammation of the pancreas (post‑ERCP pancreatitis) occurred in about 9% of patients, while minor bleeding occurred in about 4%; there were no cases of perforation, infection, or death, and all bleeding was controlled during the procedure. Strikingly, every single complication happened in the group with difficult cannulation. The longer the doctor had to work at reaching the duct and the more attempts that were needed, the higher the chance of trouble. A cannulation time of about nine minutes or more, or four or more attempts, strongly signaled increased risk of complications.
Who is most at risk among cirrhotic patients
By combining all the information, the investigators identified several key predictors of difficult cannulation in compensated cirrhosis. Older age modestly raised the odds. Certain papilla shapes (types 2 and 3) and the presence of a diverticulum near the papilla roughly doubled or more the likelihood of difficulty. The need for precut sphincterotomy—the cutting maneuver used when standard approaches fail—was the strongest predictor of all, multiplying the odds of difficult cannulation many times. Patients who smoked or had other major illnesses such as obesity, kidney disease, or autoimmune conditions were also more likely to experience complications once difficulty arose.
What this means for patients and doctors
For people with compensated cirrhosis, ERCP is often necessary and can be life‑improving, but this study shows that almost half will have a technically challenging procedure, and that difficulty is closely tied to a higher chance of pancreatitis and bleeding. In plain terms, the more the endoscopist has to "fight" to enter the bile duct—especially in older patients, those with awkwardly shaped duct openings, or nearby intestinal pouches—the more carefully the team must weigh risks, limit repeated attempts, and consider alternative strategies. While the study is from a single center and did not include patients with more advanced cirrhosis, it underscores that recognizing these warning signs before and during ERCP may help tailor the procedure, protect vulnerable patients, and guide future research on safer approaches.
Citation: Elkerdawy, M.A., Mahros, A.M., Emara, M.H. et al. Difficult biliary cannulation among patients with compensated liver cirrhosis: predictors and impact on complications. Sci Rep 16, 9533 (2026). https://doi.org/10.1038/s41598-026-41040-1
Keywords: ERCP, liver cirrhosis, bile duct, pancreatitis, endoscopy complications