Clear Sky Science · en
Comparison of compensatory strategies and gait deviations in unclassified and type 1 unilateral cerebral palsy
Why the way we walk matters
Walking is something most of us do without thinking, but for children and adults with unilateral cerebral palsy—where one side of the body is primarily affected—each step is a complex balancing act. This study explores how the body quietly “reorganizes” itself to keep people moving: the trunk, pelvis, hips, knees and ankles all adopt backup strategies to deal with a shorter or weaker leg. Understanding these hidden adjustments may help doctors design better treatments that protect joints and improve comfort and independence over a lifetime.
One-sided challenges, whole-body solutions
Cerebral palsy is a life-long condition caused by early brain injury that affects muscle control and coordination. In unilateral cerebral palsy, one leg is mainly involved, but the body is naturally asymmetric: every step depends on both legs working together. Classic medical classifications focus mostly on how the affected leg moves in a single plane—looking largely at the ankle, knee and hip from the side. Many people, however, do not fit neatly into these categories and are labeled “unclassified,” even though they clearly walk differently from typically developing peers. The authors suspected that important changes outside this narrow view—especially in the pelvis, trunk and the supposedly “sound” leg—were being overlooked.
High-tech tracking of every step
To uncover the full picture, the researchers analyzed three-dimensional walking patterns in 47 people with unilateral cerebral palsy and compared them to 26 typically developing individuals. Participants walked barefoot along a short walkway while a camera system tracked reflective markers on their trunk, pelvis and legs, and force plates measured how they pushed against the ground. The team looked at motion in all three planes—forward-and-back, side-to-side and rotational—across the entire walking cycle. They paid particular attention to differences between people with a classic “type 1” drop-foot pattern and those who were unclassified, while also noting small but important differences in leg length between sides.
Hidden asymmetries in pelvis, trunk and limbs
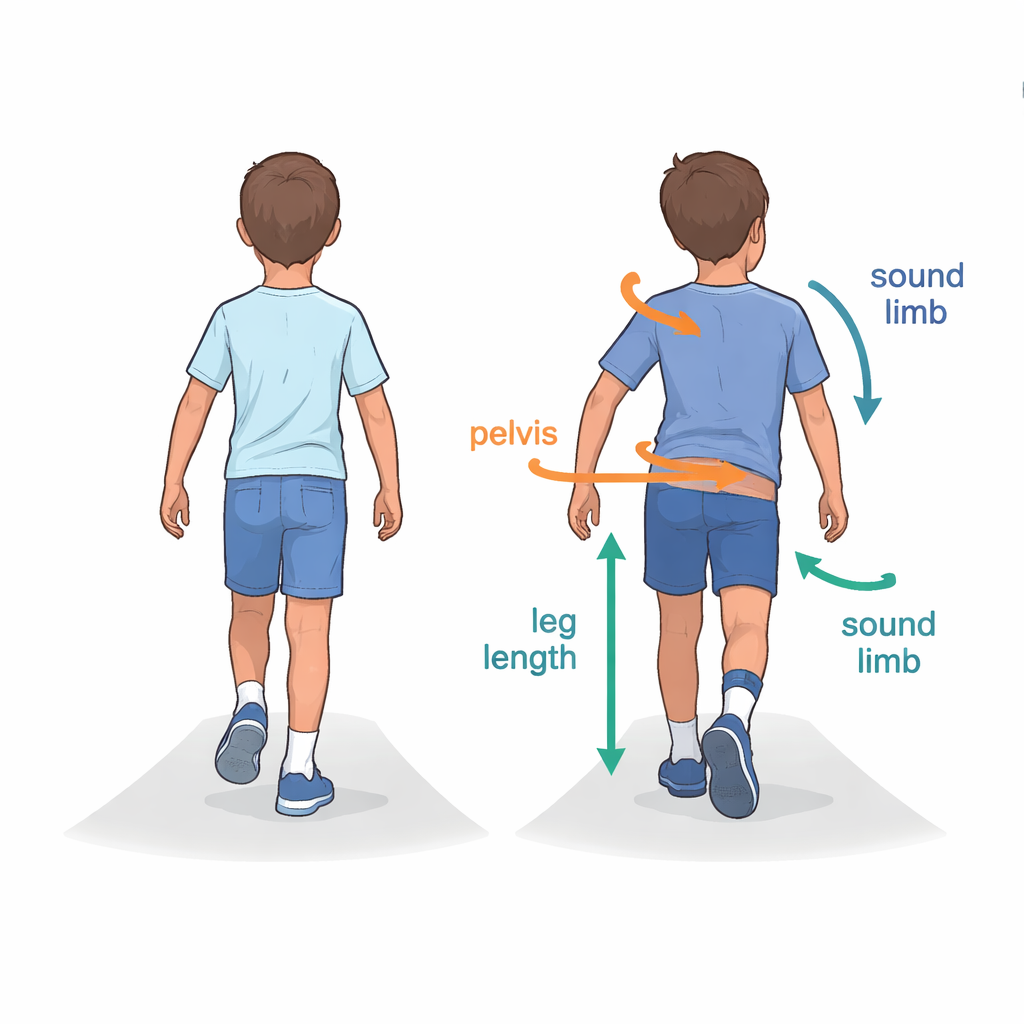
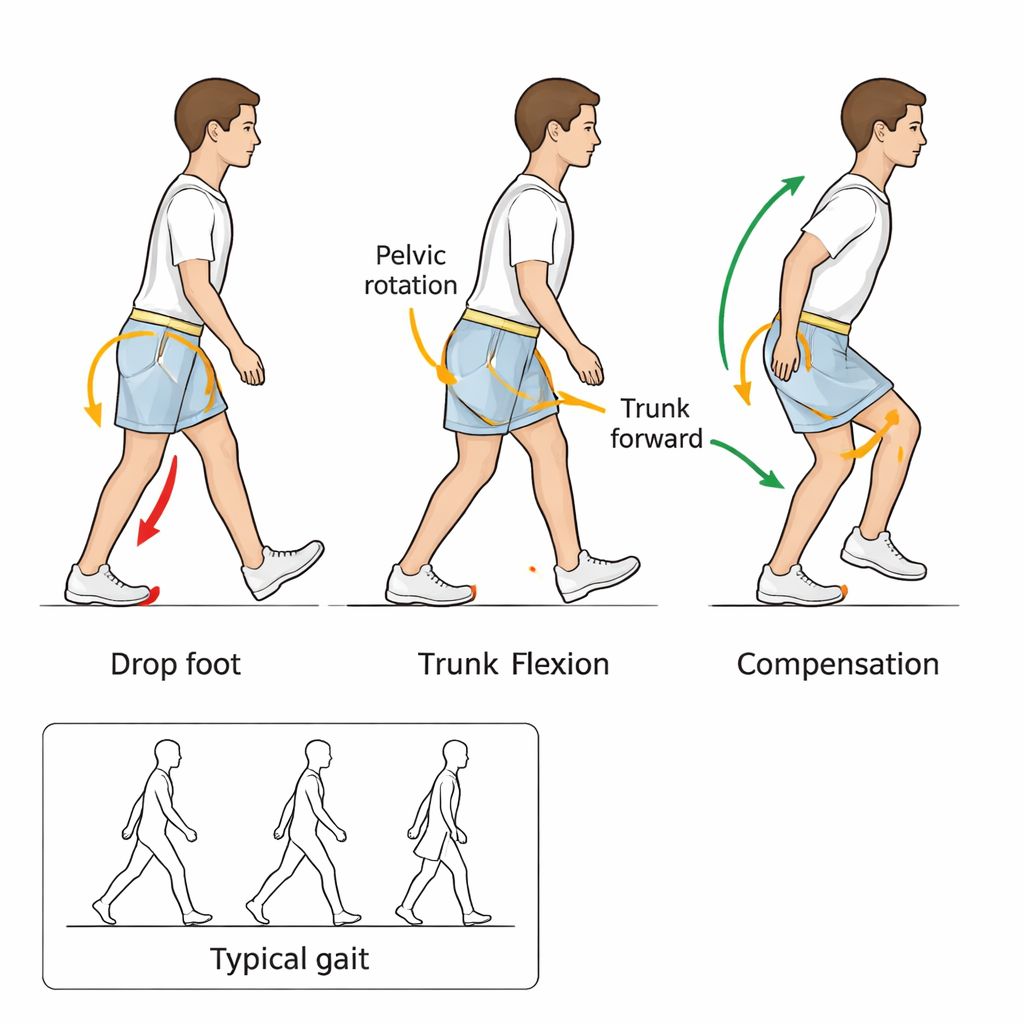
The study found that, despite their different labels, unclassified and type 1 participants shared many similar whole-body deviations when compared with typically developing walkers. Both groups showed forward-leaning trunks, tilting of the trunk and pelvis toward the affected side, and rotation of the pelvis around the body’s vertical axis. These features were closely tied to leg length differences and helped the body keep the feet pointed in a functional direction. At the joints, both legs—not just the affected one—often bent more at the hip and knee. In type 1, the affected ankle tended to point downward (a drop-foot or equinus pattern), while unclassified participants showed the opposite: extra upward bend at the ankle, resembling a crouched style of walking. Even the “good” leg was not truly normal; it frequently adopted extra flexion and subtle rotations to make up for length and alignment differences.
Why current labels miss the real problem
Because existing classification systems focus mainly on side-view ankle motion in the affected leg, they miss key drivers of abnormal gait: leg length discrepancy and twisting of the pelvis and upper body. This leaves many people in a diagnostic gray zone and may encourage treatment plans that target only the obviously affected side. The new findings suggest that rotational asymmetry—especially pelvic rotation—and the way the sound leg compensates are central features of unilateral cerebral palsy for both mildly and more clearly affected individuals. Ignoring these factors could allow excessive stress to build up in the “better” limb, possibly contributing to joint wear such as osteoarthritis later in life.
Translating motion into better care
For a layperson, the take-home message is that unilateral cerebral palsy is not just a problem of one foot or ankle; it is a whole-body adaptation to a shorter or misaligned leg. Subtle twists and tilts in the pelvis and trunk, together with extra bending in both legs, are not random quirks but deliberate strategies the body uses to stay upright and move forward. The authors argue that doctors should routinely measure pelvic rotation and leg length differences, and consider treatments that correct these, such as bone realignment surgery in selected cases. By updating classification systems to include these three-dimensional features and the behavior of the sound limb, care teams can plan more precise, individualized therapies aimed at restoring a more balanced, energy-efficient and joint-friendly way of walking.
Citation: Tsitlakidis, S., Beckmann, N.A., Weishorn, J. et al. Comparison of compensatory strategies and gait deviations in unclassified and type 1 unilateral cerebral palsy. Sci Rep 16, 7465 (2026). https://doi.org/10.1038/s41598-026-40523-5
Keywords: unilateral cerebral palsy, gait analysis, pelvic rotation, leg length discrepancy, compensatory walking strategies