Clear Sky Science · en
Clustering reveals diagnostic overlap between Still’s disease and a hyperinflammatory subset of seronegative rheumatoid arthritis
Why these joint diseases matter
Many people have heard of rheumatoid arthritis, a chronic disease that slowly damages joints. Fewer know about Still’s disease, a rare illness that can cause sudden high fevers, rashes, and inflamed joints. Doctors sometimes struggle to tell these conditions apart, especially in patients who test negative for the usual rheumatoid arthritis antibodies. This study asks a simple but important question: when symptoms blur together, are we really looking at different diseases, or at overlapping forms of the same inflammatory process?
Two illnesses with shared faces
Still’s disease is an uncommon inflammatory disorder that affects the whole body. Patients often arrive with daily spiking fevers, a salmon-colored skin rash, sore throat, and very high markers of inflammation in the blood. Joints may be painful or swollen in patterns that range from brief and mild to long-lasting and destructive. Rheumatoid arthritis, by contrast, is a common cause of chronic joint swelling and damage. In most patients, blood tests reveal specific antibodies, but about one quarter lack these markers; they are said to have “seronegative” rheumatoid arthritis. Because both Still’s disease and seronegative rheumatoid arthritis can present with joint pain and no antibodies, they can easily be confused in day-to-day practice.
How the researchers grouped patients
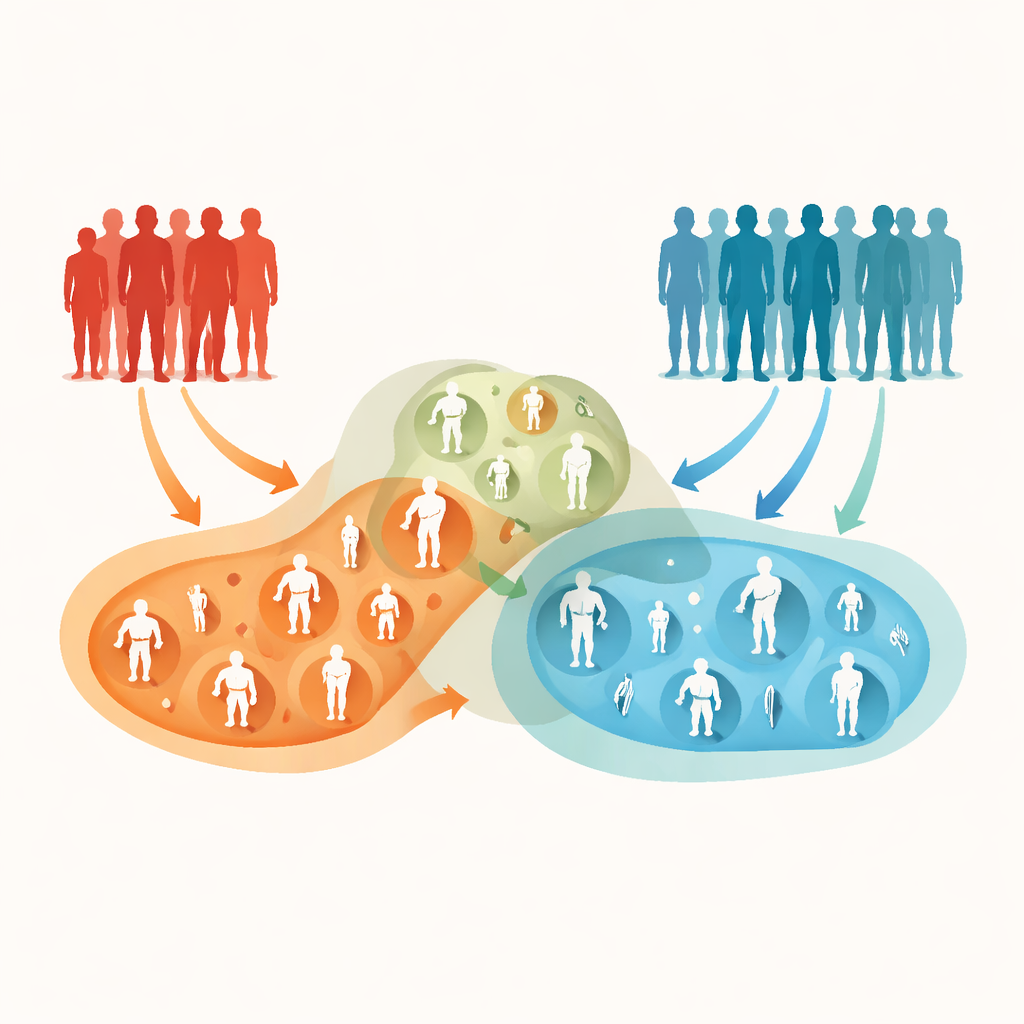
The authors analyzed medical records from 312 adults treated in French hospitals: 98 with joint-involving Still’s disease, 93 with antibody-positive rheumatoid arthritis, and 121 with seronegative rheumatoid arthritis. For each person, they gathered information from the time of diagnosis, including age, symptoms such as fever, weight loss and skin rash, details of which joints were inflamed, and blood measures of inflammation and immune activity. Instead of forcing patients into preset diagnostic boxes, they used a data-driven technique called clustering. This method looks for natural groupings in the data and arranges patients into clusters that share similar patterns of symptoms and laboratory results, without being told in advance which disease label they carry.
Three hidden patterns emerge
The computer analysis revealed three clear clusters. The first and largest contained mostly people with classic rheumatoid arthritis, both antibody-positive and seronegative. These patients tended to be older, had many small joints of the hands and feet involved on both sides of the body, and showed only modest increases in blood markers of inflammation. Autoantibodies were common in this group. The second cluster was dominated by Still’s disease. These patients were younger and arrived with striking whole-body illness: high fevers, weight loss, rash, sore throat, and very high levels of inflammation in the blood. Their joints were often widely affected, but blood tests for rheumatoid antibodies were usually negative, and many later went into remission, sometimes even without long-term treatment.
The mixed middle ground
The third, smaller cluster was the most intriguing. It contained a near-equal mix of Still’s disease and seronegative rheumatoid arthritis. These patients showed intermediate levels of inflammation. Their joint problems were fewer in number, often affecting one side more than the other, and did not fit the classic rheumatoid pattern. General symptoms like fever and rash were present but less dramatic than in the Still’s-dominated cluster. Autoantibodies were rare. This cluster hints at a blended, highly inflammatory form of arthritis that does not sit neatly in either the traditional Still’s disease or rheumatoid arthritis categories. The authors suggest that this overlap group could represent a subset they call “Systemic Inflammatory Rheumatoid Arthritis,” a label meant to capture its joint-centered but body-wide inflammatory character.
What this means for patients and doctors
To a lay reader, the key message is that not all arthritis that looks like rheumatoid arthritis truly behaves the same way. Most people with seronegative rheumatoid arthritis in this study resembled those with classic, antibody-positive disease. But roughly one in five had a picture closer to Still’s disease, with more intense inflammation throughout the body. Recognizing this overlap matters, because these patients may benefit from treatments that target the powerful inflammatory pathways active in Still’s disease, and they may need especially careful evaluation before a firm label is applied. The authors stress that their findings are hypothesis-generating rather than practice-changing; larger, forward-looking studies and biological tests are needed to confirm whether this mixed cluster is truly a distinct disease type. Still, their work shows how modern data analysis can uncover hidden patterns in familiar illnesses, and may eventually lead to more tailored care for people living with severe inflammatory arthritis.
Citation: Mercier-Guery, A., El-Jammal, T., El-Nayef, N. et al. Clustering reveals diagnostic overlap between Still’s disease and a hyperinflammatory subset of seronegative rheumatoid arthritis. Sci Rep 16, 10339 (2026). https://doi.org/10.1038/s41598-026-40493-8
Keywords: Still’s disease, seronegative rheumatoid arthritis, inflammatory arthritis, disease clustering, hyperinflammation