Clear Sky Science · en
Efficacy of fully covered self-expanding metal stents removal versus stent-in-stent techniques in recurrent malignant distal biliary obstruction
Why blocked bile ducts matter
When cancers of the pancreas or bile ducts grow, they can squeeze the tiny tube that drains bile from the liver into the intestine. This blockage leads to jaundice, infection, and severe itching, and it can keep patients from receiving further cancer treatment. Doctors often keep this passage open by placing tiny metal tubes called stents. As people with these cancers live longer thanks to better drugs, those stents have more time to clog or shift, raising a new question: what is the best way to fix a failing stent?
Two main ways to fix a failing tube
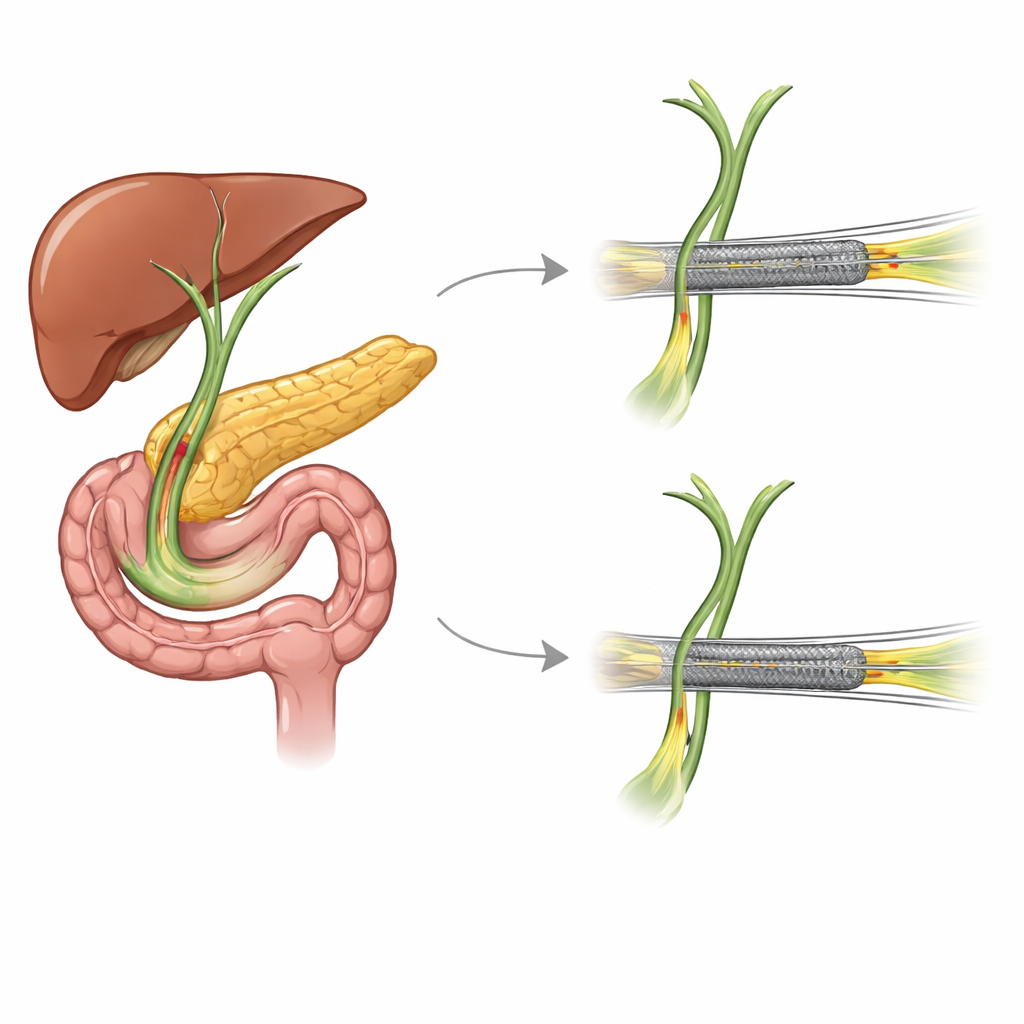
This study followed 159 patients in South Korea with advanced cancers causing blockage near the end of the bile duct. All were first treated with a fully covered metal stent, which can later be removed. When that first stent eventually failed, doctors chose between two main strategies. One option was to pull the old metal stent out and insert a new stent in its place (“stent exchange”). The other was to leave the old stent where it was and slide a new stent inside it (“stent-in-stent”). In both strategies, the replacement could be either another metal stent or a simpler plastic one.
Who the patients were and how they were treated
The patients, most in their seventies, mainly had pancreatic cancer, with smaller numbers affected by bile duct or ampullary cancers. They were treated at several large hospitals, and all procedures were guided by endoscopy, where doctors navigate a flexible camera from the mouth to the small intestine to reach the bile duct opening. The researchers compared four groups: metal stent exchange, plastic stent exchange, metal stent-in-stent, and plastic stent-in-stent. Importantly, all four approaches worked in the short term: doctors were able to place the stents successfully, and jaundice improved in every group.
How long the stents lasted and what went wrong
The team focused on how long each new stent stayed open before blocking again. The first stent lasted about five months on average, regardless of how it was later revised. But the second stent told a different story. When doctors removed the old covered metal stent and replaced it with a new metal stent, the second stent stayed open the longest, around five to six months on average. Stent-in-stent approaches and plastic replacements failed sooner. Advanced statistical tests showed that leaving the old metal stent in place and placing a new metal stent inside it increased the risk of another blockage more than sixfold compared with full metal stent exchange. Plastic stents, whether exchanged or used in a stent-in-stent pattern, also carried higher risks of early re-blockage.

Safety, survival, and timing
Despite these differences in how long the stents stayed open, patients lived for similar lengths of time no matter which revision method they received. Survival was driven more by factors such as how advanced the cancer was, whether patients could receive chemotherapy, and how high their bilirubin levels were at the start. Complications like infections and pancreatitis occurred at similar rates in all groups, suggesting that the safer choice for keeping the duct open longer—metal stent exchange—did not come with extra short-term risks. The study also found that if the first stent failed early, within about six months, patients were more likely to face another blockage after revision, hinting that aggressive disease or difficult anatomy may make long-term drainage harder to achieve.
What this means for patients and doctors
For people living with advanced pancreatic and bile duct cancers, this study suggests a clear practical message. When a fully covered metal stent that was placed to relieve bile duct blockage fails, taking it out and inserting a new metal stent in its place appears to keep the duct open longer than simply stacking a new stent inside the old one or switching to a plastic tube. This approach does not seem to shorten overall survival or add extra danger, but it may reduce the number of times patients need to return for repeat procedures. As cancer drugs continue to extend life, choosing the stent strategy that offers the longest, most reliable relief from bile duct blockage will be increasingly important for comfort and for keeping treatment options open.
Citation: Lee, S.Y., Jang, S.I., Kim, E.J. et al. Efficacy of fully covered self-expanding metal stents removal versus stent-in-stent techniques in recurrent malignant distal biliary obstruction. Sci Rep 16, 10408 (2026). https://doi.org/10.1038/s41598-026-40409-6
Keywords: bile duct stent, pancreatic cancer, biliary obstruction, endoscopic drainage, metal versus plastic stents