Clear Sky Science · en
Intercostal thickening fraction adds no value to diaphragm thickening fraction in healthy subjects undergoing noninvasive ventilation
Why breathing effort matters
When people struggle to breathe, doctors often turn to noninvasive ventilation—a tight-fitting mask connected to a machine—to help push air into the lungs without inserting a breathing tube. But setting the machine correctly is a delicate balancing act: too little support leaves patients fighting for breath, while too much can injure the lungs or weaken the breathing muscles. This study asks a simple but important question: can a quick ultrasound scan of the chest reliably show how hard someone is breathing, and do we gain anything by looking at more than one set of muscles?
The main breathing muscle under the spotlight
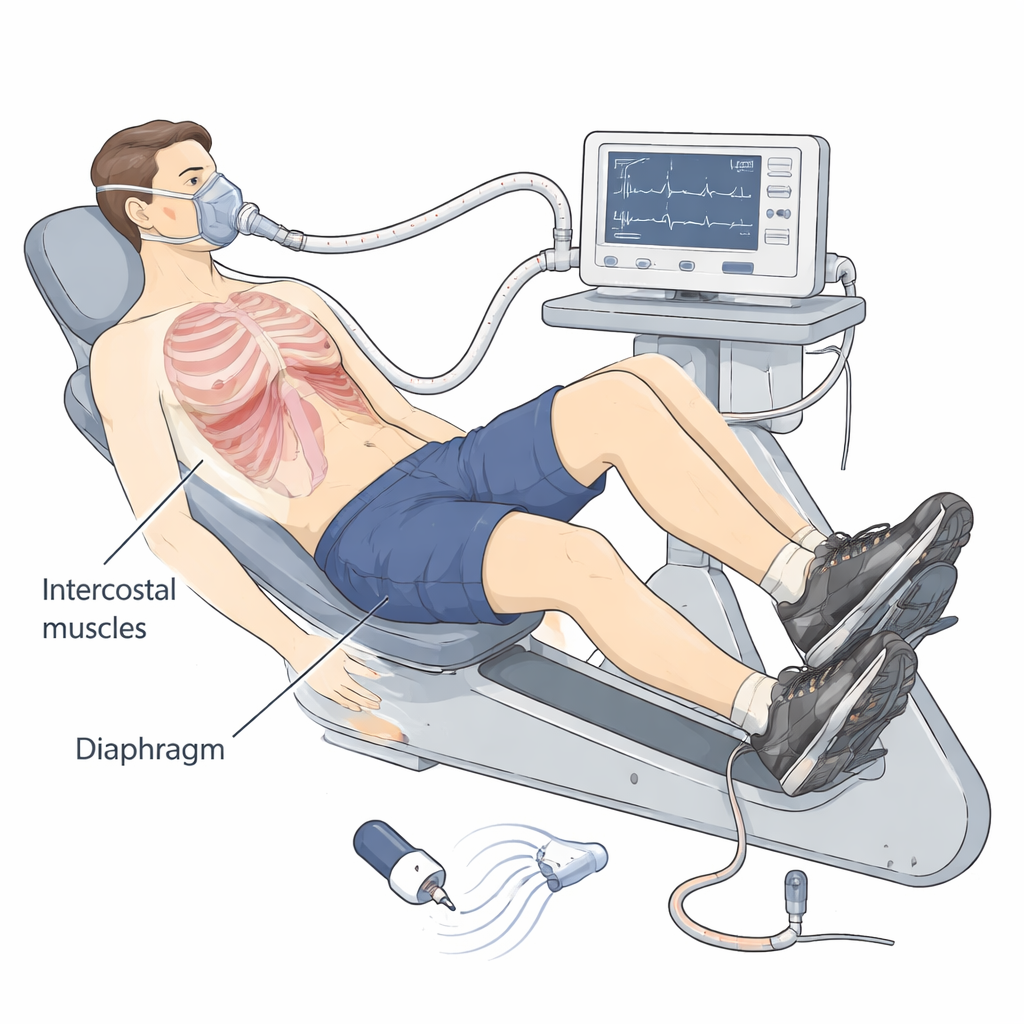
The diaphragm, a dome-shaped sheet of muscle under the lungs, is the workhorse of normal breathing. As it tenses, it thickens and moves downward, drawing air into the chest. Earlier work suggested that measuring how much the diaphragm thickens with each breath—called the diaphragm thickening fraction—might reflect how hard a person is working to breathe. To test this idea in a controlled way, the researchers recruited 38 healthy young adults and asked them to pedal on a semi‑reclined exercise bike while wearing a breathing mask connected to a ventilator.
Putting breathing muscles to the test
Each volunteer completed three exercise levels: resting, light effort, and hard effort, based on how strenuous the activity felt. Within each exercise level, the ventilator settings were shuffled in random order, ranging from no machine support to increasingly higher pressure support. At every stage, the team measured three things: how much the diaphragm thickened on ultrasound, how much the small muscles between the ribs near the breastbone (the parasternal intercostals) thickened, and how much the pressure inside the chest changed with each breath. That pressure change, measured with a thin balloon catheter in the esophagus, is considered a gold-standard indicator of breathing effort, but it is invasive and uncomfortable.
What the measurements revealed
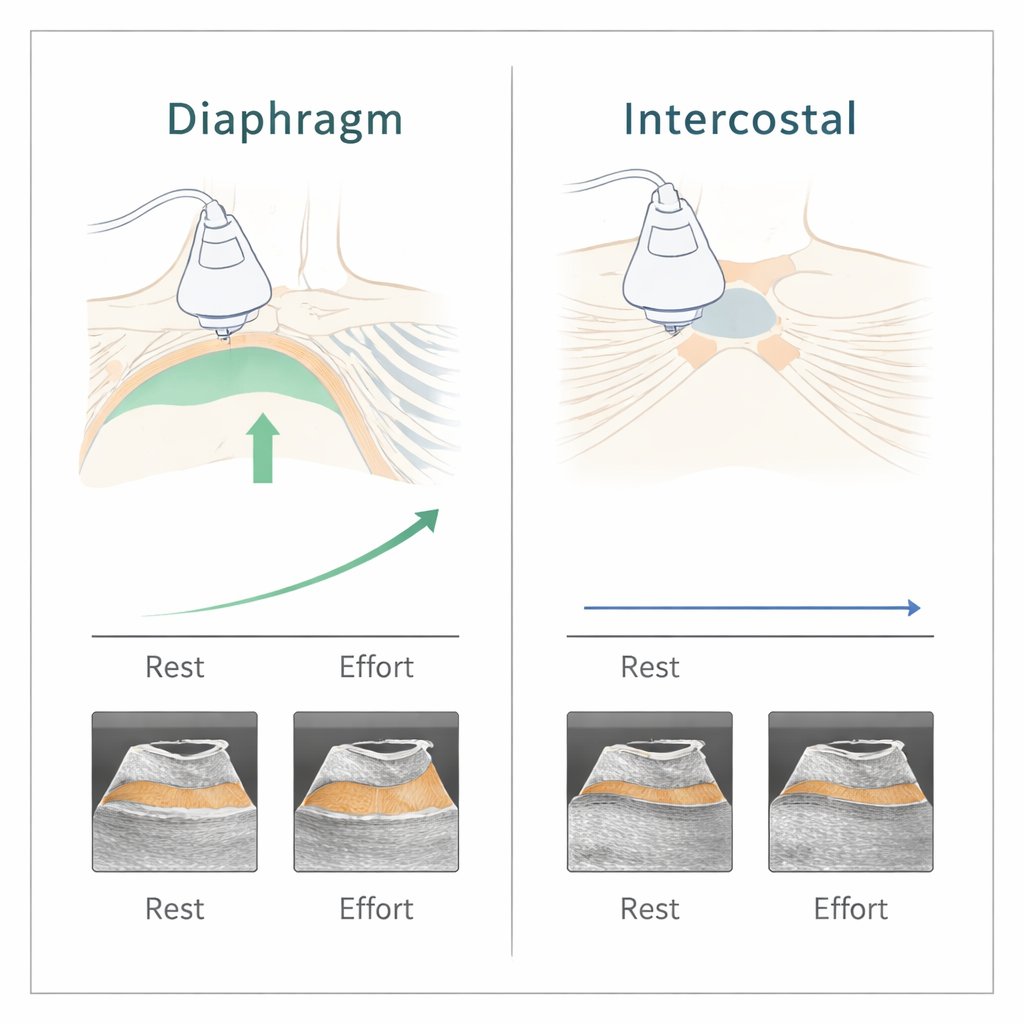
As exercise intensity rose, both the diaphragm thickening and the pressure swings inside the chest became larger, meaning that volunteers were indeed working harder to breathe. Statistical analysis showed a moderate link between diaphragm thickening and the pressure swings across all the different ventilator settings. In other words, when breathing effort went up or down, the diaphragm ultrasound tended to move in the same direction. The pressure catheter still did a better job of separating the different exercise levels, but diaphragm ultrasound could distinguish them reasonably well too.
Why rib muscles did not add much
The story was very different for the intercostal muscles near the breastbone. Their thickness barely changed with either exercise or different ventilator settings, and their measurements did not track with the pressure swings or with diaphragm thickening. In this group of healthy adults with normal diaphragm function, scanning these rib muscles simply did not provide useful extra information. One likely reason is that these muscles help stabilize the rib cage rather than shortening dramatically with each breath, so their thickness on ultrasound may not change much except during extreme breathing efforts or when the diaphragm is weak.
What this means for real‑world care
For everyday practice, these findings suggest that a simple ultrasound of the diaphragm could help clinicians gauge relative changes in breathing effort and adjust noninvasive ventilator settings more confidently, while sparing patients the discomfort of an internal pressure catheter. At least in healthy individuals, adding ultrasound of the parasternal intercostal muscles does not improve this assessment. The authors caution that their work was done in young, healthy volunteers under tightly controlled conditions, not in sick patients. Future studies in people with lung disease or weakened diaphragms will be needed to see whether rib muscle measurements become more informative when the main breathing muscle can no longer carry the load.
Citation: Hoermann, C., Drotleff, L.S., Link, B. et al. Intercostal thickening fraction adds no value to diaphragm thickening fraction in healthy subjects undergoing noninvasive ventilation. Sci Rep 16, 7165 (2026). https://doi.org/10.1038/s41598-026-40192-4
Keywords: noninvasive ventilation, diaphragm ultrasound, respiratory effort, breathing muscles, critical care