Clear Sky Science · en
DGOU classification guided cement diffusion strategy in unilateral kyphoplasty for osteoporotic vertebral compression fractures
Why broken back bones matter in aging
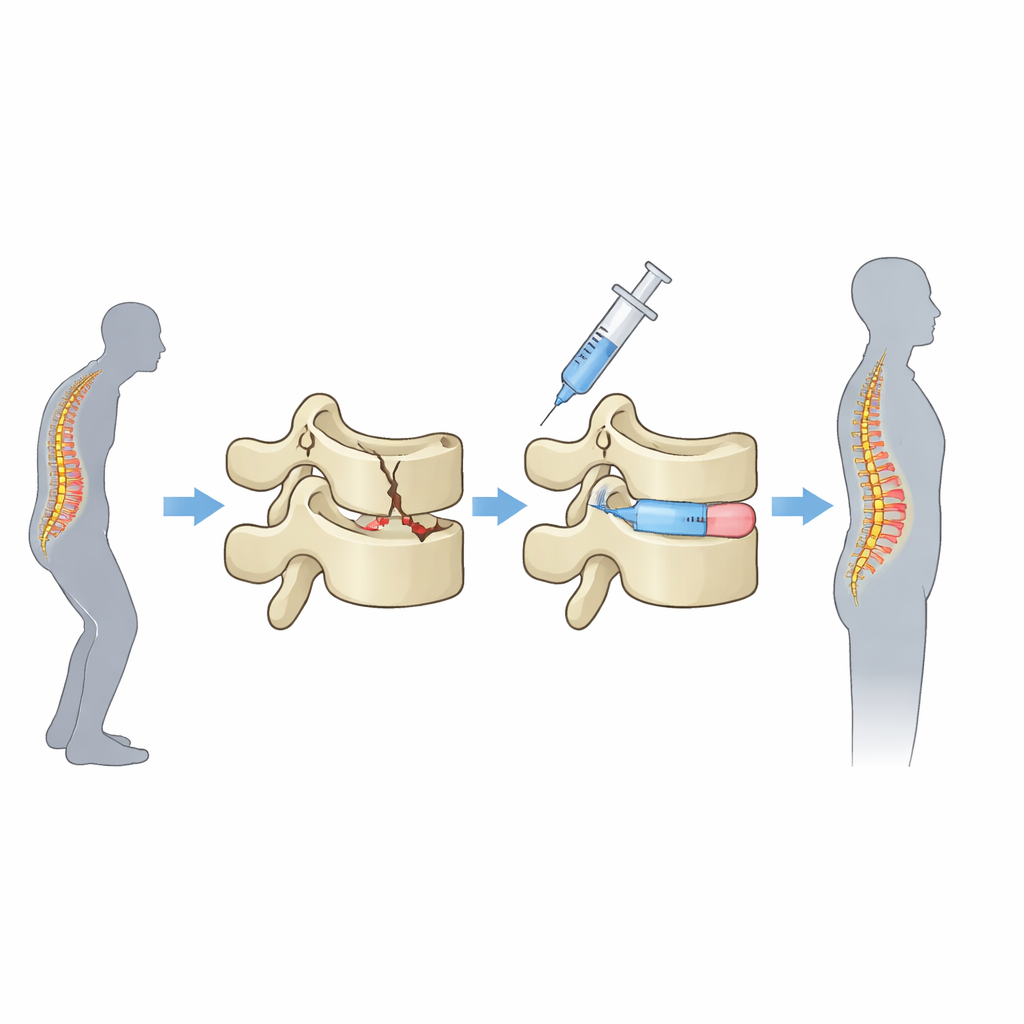
As people age, their bones often become thinner and more fragile, a condition known as osteoporosis. In the spine, this can lead to tiny breaks that crush a vertebra, causing sudden back pain, loss of height, and a hunched posture. A common minimally invasive treatment injects medical cement into the broken bone to stabilize it. But surgeons still debate a basic question: when cement is injected from one side, does it really need to spread all the way across the vertebra, or is filling one side enough? This study tackles that question and offers practical guidance for tailoring surgery to the type of fracture.
How doctors fix crushed spine bones
The operation studied here is called percutaneous kyphoplasty. Through a small skin puncture on one side of the back, surgeons pass a needle into the damaged vertebra, inflate a tiny balloon to help restore height, remove the balloon, and then inject a thick bone cement. The cement quickly hardens, acting like an internal cast that reduces painful movement and helps the bone carry weight again. Because the puncture is made from only one side, the cement may either stay mostly on that side or diffuse across the middle of the vertebra and form a more even, bridge-like support inside.
Sorting fractures by how unstable they are
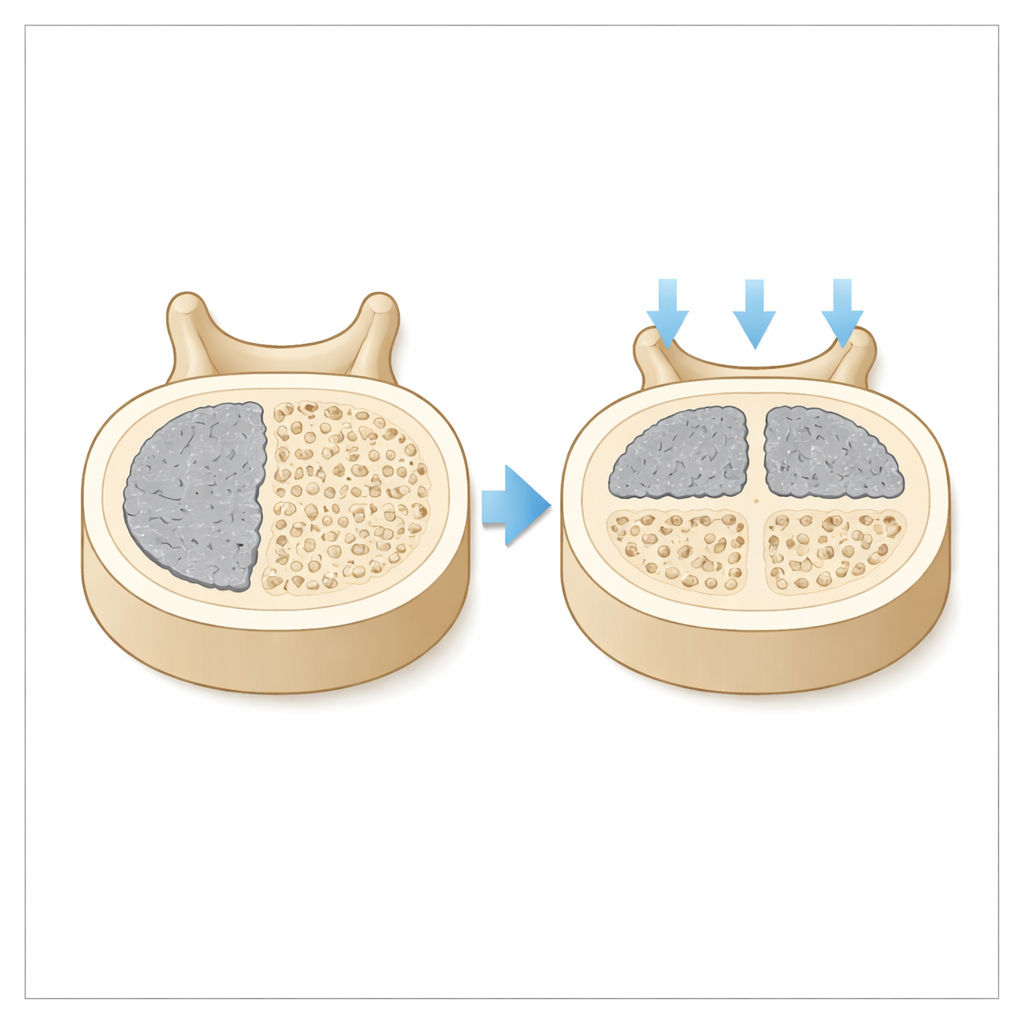
The researchers used a stability-based system called the DGOU classification to divide 440 patients with a single osteoporotic spinal fracture into three groups. OF1 fractures are relatively stable wedge cracks without major collapse; OF2 fractures have damage to the back wall of the vertebra and are potentially unstable; OF3 fractures are burst-type breaks that are clearly unstable. All patients had unilateral kyphoplasty at four hospitals between 2020 and 2023 and were followed for at least a year. After surgery, detailed CT scans and 3D computer models were used to measure how much cement crossed the midline of the vertebra. Patients were then labeled as having either non-crossing cement (mostly on the puncture side) or cross-midline cement (a substantial portion extending to the opposite side).
Who really needs cement to cross the middle
The team tracked pain scores, daily function, and X‑ray measurements of vertebral height and spinal curve over 12 months. For the most stable OF1 fractures, outcomes were similar whether or not the cement crossed the midline: patients experienced strong pain relief, better function, and good maintenance of vertebral shape with either pattern. In contrast, for OF2 and OF3 fractures, a clear pattern emerged. When cement spread across the vertebra, patients had better function scores from one month onward and maintained vertebral height and spinal alignment more effectively over time. Importantly, achieving cross-midline spread required a slightly wider needle angle and somewhat longer surgery, but it did not require more cement and did not increase serious complications such as leakage of cement or new fractures in neighboring vertebrae.
Why symmetry inside the bone matters
The authors argue that the key is how much the original structure of the vertebra has been weakened. In stable OF1 fractures, the central part of the bone still carries load fairly well, so a solid “plug” of cement on one side is enough to stop painful micromovement. In the more damaged OF2 and OF3 fractures, however, the middle of the vertebra is compromised, and the bone is prone to collapsing further. In that setting, leaving cement on only one side can create uneven forces, like standing on the edge of a broken stepping stone. Spreading cement across the midline builds a more balanced internal scaffold that shares weight evenly and better resists gradual collapse and increased spinal curvature.
What this means for patients and surgeons
Put simply, the study suggests that not all osteoporotic spine fractures should be treated the same way. For milder, more stable fractures, surgeons performing unilateral kyphoplasty do not need to chase cement across the vertebra, which can keep the procedure shorter and simpler without sacrificing benefit. For more serious, unstable fractures, however, working to achieve a cross-midline cement pattern appears worthwhile: patients move better, their vertebrae keep their shape longer, and these gains come without added safety risks when the technique is used carefully. Using the DGOU fracture type as a guide, the authors recommend setting different cement-spread goals for different fracture severities, helping move spinal fracture care toward more precise, individualized treatment.
Citation: Cao, D., Li, X., Gu, W. et al. DGOU classification guided cement diffusion strategy in unilateral kyphoplasty for osteoporotic vertebral compression fractures. Sci Rep 16, 9281 (2026). https://doi.org/10.1038/s41598-026-40167-5
Keywords: osteoporotic vertebral compression fracture, percutaneous kyphoplasty, bone cement distribution, spinal fracture stability, DGOU classification