Clear Sky Science · en
Propensity score-matched analysis of percutaneous endoscopic versus conservative treatment for lumbar disc herniation in high-risk octogenarians
Why this matters for aging families
More and more people are living into their late eighties and beyond, but many of them are held back by crippling low back and leg pain from slipped discs in the spine. For these fragile adults, full open back surgery can be risky, while months of medicines and therapy often do not bring enough relief. This study asks a practical, family-centered question: for very old, medically complex patients, is a tiny "keyhole" spine procedure done under local numbing medicine a safer and more effective way to get them back on their feet than continued non-surgical care?
A tough problem in the oldest-old
People aged 85 and older are the fastest-growing age group worldwide, and many suffer from lumbar disc herniation, where a worn spinal disc presses on a nerve and causes sharp leg pain, weakness, and loss of independence. Treating them is difficult because they often have heart disease, lung problems, diabetes, and overall frailty that make standard operations and general anesthesia dangerous. At the same time, simply relying on pain pills, physical therapy, and injections can leave them stuck in bed or in a chair, which in turn worsens muscle loss, fall risk, and even memory. Doctors need options that relieve pressure on the nerves without overwhelming an aging body. 
A small opening and a big team
The researchers focused on a minimally invasive technique called percutaneous endoscopic transforaminal discectomy. Instead of a large incision and muscle stripping, surgeons make a cut only about a centimeter long in the lower back, slide a narrow tube to the problem disc, and use a camera and tiny tools to remove the offending tissue. Crucially, this is done under local anesthesia, so the patient stays awake and can alert the team if a nerve is irritated. Around this operation sits a multidisciplinary team: geriatricians assess frailty and medicines, heart and lung specialists fine-tune circulation and breathing, diabetes experts manage blood sugar, and anesthesiologists oversee gentle sedation and monitoring. Together they aim to turn many "too risky" older patients into candidates for a short, targeted procedure.
Comparing surgery to non-surgical care
To make a fair comparison, the authors looked back at 64 ultra-elderly patients (average age about 89) who had this keyhole procedure and matched them to 64 similar patients who had chosen or been steered toward conservative treatment. Matching took into account age, sex, body size, number of other illnesses, level of disc damage, pain scores, disability scores, and measures of frailty. The non-surgical group received a thorough program of medicines, physical therapy, traction, injections, and lifestyle advice for at least three months, with surgery only considered later if pain remained severe or function declined further.
Pain relief, mobility, and safety
Over roughly a year of follow-up, the differences were striking. Those who had the endoscopic procedure reported far larger drops in back and leg pain and much better scores for everyday activities like walking, dressing, and self-care. By the study’s final check, about 95 percent of operated patients rated their outcome as excellent or good, compared with only about one-third of those managed without surgery. More than a quarter of the conservative group eventually needed an operation anyway because symptoms persisted or worsened, while none of the keyhole-surgery patients required a repeat procedure. With team-based preparation, most patients had their medicines optimized beforehand, stood up for the first time just a few hours after surgery, and went home after a little over two days. Importantly, there were no serious complications such as infections, nerve damage, heart attacks, or lung crises, and no flare-ups of existing medical problems. 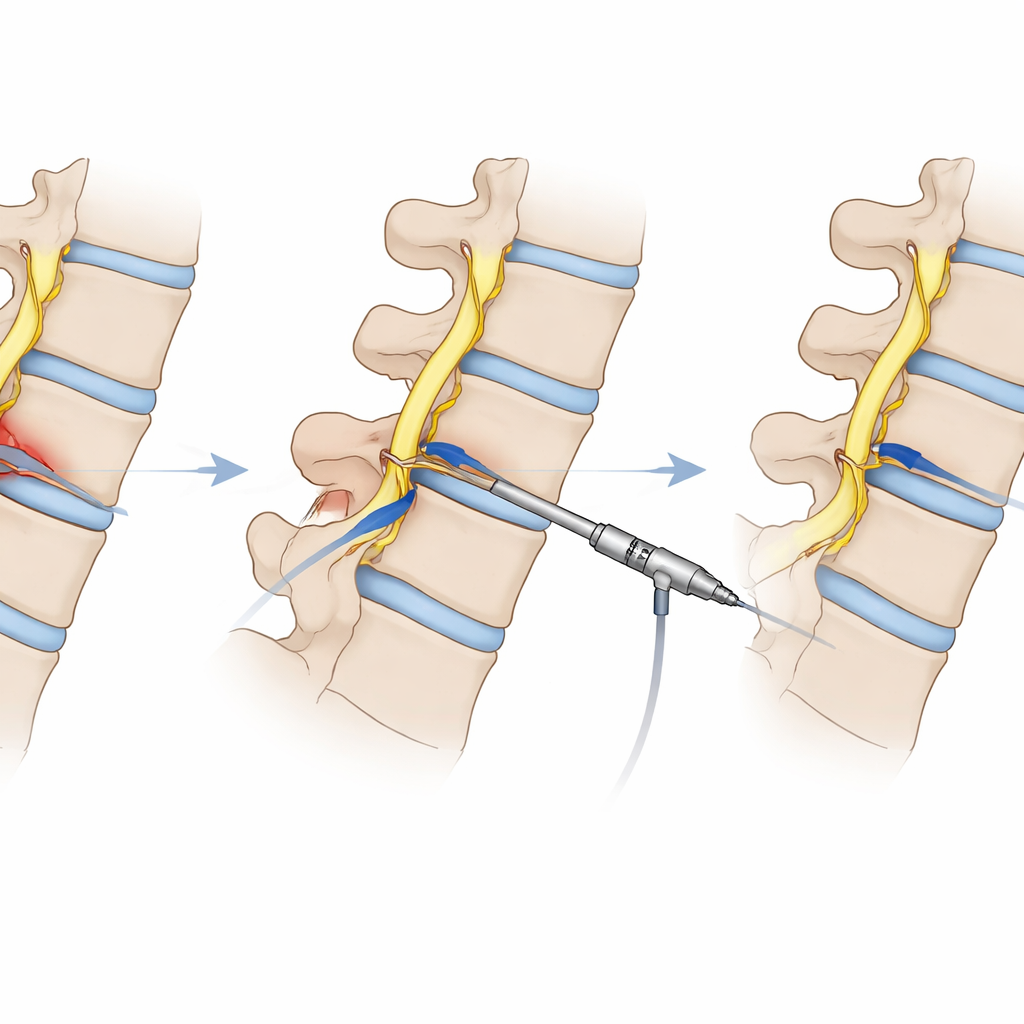
Rethinking when to avoid or delay surgery
The study also challenges the common belief that very advanced age plus multiple illnesses automatically rule out spine surgery. The authors argue that with careful team review, age and comorbidities become factors to manage rather than hard stop signs. They note that repeatedly postponing intervention while trying one non-surgical step after another may backfire in the oldest-old, allowing pain, immobility, and frailty to spiral. In this group, a short, focused procedure that quickly restores walking may be kinder to the body than months of ongoing suffering.
What this means for patients and families
For families caring for relatives in their late eighties and beyond, this research offers cautious optimism. It suggests that, when delivered within a coordinated medical team and under local anesthesia, a tiny endoscopic operation on the lower spine can provide much better pain relief, function, and independence than prolonged conservative care, without adding serious risk. While the study is retrospective and covers only about a year of outcomes, it supports viewing keyhole spine surgery as a realistic, everyday tool to balance effective nerve decompression with the delicate health of the oldest-old.
Citation: OuYang, B., Sun, H., Zhang, K. et al. Propensity score-matched analysis of percutaneous endoscopic versus conservative treatment for lumbar disc herniation in high-risk octogenarians. Sci Rep 16, 8322 (2026). https://doi.org/10.1038/s41598-026-39853-1
Keywords: lumbar disc herniation, elderly spine surgery, minimally invasive back procedure, local anesthesia, multidisciplinary care